2622143
Description
Flashcards by Sameet Govan, updated more than 1 year ago
|
|
Created by Sameet Govan
almost 9 years ago
|
|
| Question | Answer |
| Dual platelets to use following and MI | Ticagrelor OR Prasugrel And aspirin |
| NYHA classification of heart failure | 1 - asymptomatic 2 - shopping around ASDA 3 - put bin out 4 - symptoms at rest, get out of bed and sit in chair |
| Causes of raised BNP | Heart failure AF or increased HR LVH Age >70 COPD CKD - not excreting it |
| MI drugs | Dual anti platelet Fondaparinux beta blocker statin Acei |
| CHADSVASC 2 score for? | risk of stroke in AF |
| Lipid risk scores, Qrisk 2 and JBS2 | 10 year risk percentage of cardiovascular event At 10% you can offer treatment Statin or ezetimibe primary prevention atorvastatin 20mg and secondary prevention - atrovastatin 80mg Also offer statin in type 1 diabetes if: -are older than 40 years or -have had diabetes for more than 10 years or -have established nephropathy or -have other CVD risk factors. Offer it in those with CKD for primary and secondary prevention. |
| HAS-BlED | estimates major bleeding when on anti-coagulation for AF |
| Broad complex regular tachycardia is what | VT until proven otherwise Could also be AF with aberrant conduction or LBBB |
| Causes of narrow complex regular tachycardia | Sinus tachycardia, AV nodal tachycardia, atrial flutter, atrial tachycardia, AV re-entrant tachycardia - in WPW |
| Narrow complex irregular tachycardia | AF AF with variable block Multifocal atrial tachycardia |
| Wide complex irregular tachycardia | Any irregular supra ventricular tachycardia with aberrant conduction Any irregular super ventricular tachycardia with pre-existing bundle branch block AF with WPW syndrome polymorphic ventricular tachycardia |
| What would the p wave look like in lead II in a junctional rhythm | Inverted |
| How to diagnose right ventricular hypertrophy on ECG | Dominant R wave in V1, R axis deviation, P pulmonale + normal width QRS, deep S wave in V6, severe cases T wave inversion |
| Intermittent RBBB, why? | called aberration Mechanism is that RBB and LBB have different refractory periods, LBB is shorter so at certain rates there is an RBBB an some impulses only transmitted through LBB |
| Leads to look for LVH strain | Sagging QT in V5 and V6 |
| What happens in AVNRT and features of it | Depolarisation of ventricles but goes back up the node to depolarise the atria and works in a reentry way to propogate 80% cannot see a p wave 20% might see a QRS right after Can see Inverted p waves right after QRS |
| What happens in an escape rhythm | T wave then pause a no SA node depolarisation. Then something else takes over after the pause and then resumes as normal |
| What is it called when the heart is controlled by a ventricular rhythm which is faster than in heart block | accelerated idioventricular rhythm often associated with acute MI, appearance similar to VT but actually benign and should not be treated Do not diagnose VT unless HR >120 |
| Difference between extrasystole and an escape beat | Extrasystole comes early Escape beat comes late |
| Compensatory pause in what? | extrasystoles |
| Out of atrial flutter, AVNRT and AVRT, which is the most common | AVNRT |
| What is sick sinus syndrome | A disease characterised by abnormal sinus node functioning with resultant bradycardia and cardiac insufficiency Variable ECG abnormalities: Sinus Bradycardia. Sinus Arrhythmia — associated with sinus node dysfunction in the elderly in the absence of respiratory pattern association. Sinoatrial Exit Block. Sinus Arrest — pause > 3 seconds. Atrial fibrillation with slow ventricular response. Bradycardia – tachycardia syndrome |
| Causes of clockwise rotation | Right ventricular hypertrophy Lead placement |
| When is a T wave tall | When it is more than 2/3rds of the R |
| Things that can happen at a rapid access chest pain clinic based on coronary risk | Blood tests and chest X-ray An Exercise ECG test which involves walking on a treadmill at increasing speed while your pulse, blood pressure and heart trace are monitored by a cardiac technician. In case you need this test please wear loose clothing, with an easily removable top and trainers or flat shoes - no high heels or sling back shoes CT calcium scoring ( a very short CT scan (X-ray) CT coronary angiogram (an outpatient X- ray of the arteries of the heart) Echocardiogram (an ultrasound of the heart) Stress echocardiogram (a specialised heart ultrasound during exercise ) Myocardial perfusion scan ( a special heart muscle X ray – out patient test) 24hr ECG (a heart rhythm recording for 24hr. you take a small recording box home) Coronary angiogram ( see separate info sheet- an inpatient X-ray of the heart arteries) |
| Where is pericarditis pain and where does it radiate to | Central, radiates to shoulders (trapezius ridge pain) |
| Initial investigation in ACS | ECG 12 hr Trop T or I FBC and other bloods hyperglycaemia CXR |
| Management of ACS in first 12 hours | ABCDE Continuous cardiac monitoring 300mg Aspirin, clopidogrel Glycoprotein IIb/IIIa receptor antagonists in high risk NSTEMI - eptifibatide, tirofiban or abciximab Anticoagulants in ischaemic changes or elevated cardiac markers - LMWH (dalteparin) or fodaparinux (8 days, hop discharge or coronary revascularisation) Beta blockers glycaemic control |
| Time limit for when you would use thrombolysis instead | 120 mins of ECG diagnosis |
| When is a rescue PCI used | STEMI that fails to reperfuse following thrombolysis |
| in addition to long term aspirin, what and how long do you give other anticoagulants for | clopidogrel or ticagrelor for 12 months |
| When to give ACEi in MI | Long term, as soon as haemodynamically stable |
| When to give an aldosterone receptor antagonist such as epleronone | MI complicated by LV dysfunction (ejection fraction less than 0.4) in presence of clinical signs of heart failure or diabetes mellitus --> long term eplerenone |
| Hypoxia and shock in ACS | Cardiogenic pulmonary oedema and hypoxia, can eventually go to NIV Can volume load in ACS with hypotension and cariogenic shock |
| In angina history when to offer angiography | When not satisfactorily controlled by medication when you have newly diagnosed stable angina and: When coronary artery disease risk is 61-90% (can use NICE risk table) IF coronary revascularisation is being considered and invasive angio is acceptable |
| What tests to do in 30-60% risk of coronary artery disease in chest pain | 'functional imaging' |
| what to do in 10-29% Likelihood of coronary artery disease | CT calcium scoring (score based on the amount of calcium on a CT scan) if 0 then consider other causes of chest pain 1-400 offer 64-slice or above CT coronary angiography >400 offer invasive coronary angio |
| Examples of non-invasive functional imaging | myocardial perfusion scintigraphy with single photon emission CT Stress echo First pass contrast enhanced MR MR imaging |
| Secondary prevention of CV disease in angina | Aspirin 75mg daily ACEi for people with stable angina and diabetes Statin Blood pressure |
| Drugs for angina | GTN to relieve attacks Beta blocker or calcium channel blocker first line (modified release dihydropiridine e.g. nifedipine) -if poor response then go to max dose If cannot use the above then consider one of the following as mono therapy (these can also be added for dual therapy) Long acting nitrate (isosorbide mononitrate, ivabradine, nicorandil, ranolazine Consider a third drug if awaiting revascularisation or revascularisation not acceptable beta-blockers should not be prescribed concurrently with verapamil (risk of complete heart block) |
| Cardiac syndrome X | angiographically normal coronary arteries and continuing anginal symptoms, consider a diagnosis of cardiac syndrome X Continue drug treatment if it improves symptoms |
| Score and risk stratification for considering angio revascularisation | GRACE, SYNTAX or EuroScore |
| Coronary artery disease can be scored using... | SYNTAX |
| What should you refer most people to who have had a MI, heart surgery or procedure | Cardiac rehab |
| Right hear failure vs L heart failure | R heart failure - raised JVP and oedema L heart failure - raised pulmonary capillary pressure and breathlessness |
| ALternative cause of fluid overload in suspected heart failure | Renal failure |
| Treatment of HF | Drugs - diuretic, ACEi and/or ARB, beta blocker, aldosterone receptor antagonist (unless on ACEi and ARB) AF - warfarin or digoxin LBBB - consider cardiac resynchronisation therapy LVEF <35% - consider ICD unless pt die of HF or other disease in 5 years |
| How heart failure can be classified based on ejection fraction | HF with reduced ejection fraction HF with preserved ejection fraction |
| When to refer heart failure | Transthoracic doppler 2D echo and specialist assessment Refer for the above also if BNP >400 pg/ml or NTproBNP level above 2000 pg/ml BNP 100-400 or NTproBNP 400-2000 in 6 weeks |
| Relevance of serum BNP <100 or NT proBNP <400 | unlikely to be heart failure |
| How to grade symptomatic limitation of heart failure | NYHA I-IV |
| At what NYHA level is spironolactone considered | III-IV |
| When to use digoxin in heart failure | Severe or worsening LVSD despite first and second line treatment |
| How to diagnose hypertension | 3 clinic readings over 140/90 --> ambulatory BP monitoring (ABPM) or home BP monitoring over 135/85 In the mean time look for end organ damage - LVH, CKD, hypertensive retinopathy |
| testing for end organ damage in hypertension | urine for albumin creatinine ratio Bloods for kidney and lipids examine fundi 12 lead ECG |
| What is hypertension a risk factor for | CVA CAD heart failure CKD peripheral vascular disease dementia AF eye disease |
| BP aims for those aged 80 and over | clinic BP 150/90 ABPM or HBPM - 145/85 |
| Thiazide diuretics to offer instead of bendroflumethiazide | Chlortalidone or indapamide |
| Drugs that are bad in asthma | NSAIDs, Aspirin, beta blocker |
| When do you have critical limb ischaemia | Limb with ischaemic rest pain and/or tissue loss (ulcers or gangrene) that unless revascularised will result in limb loss |
| How to calculate ankle brachial index pressure for estimating risk of peripheral artery disease | BP at the ankle divided by BP and the brachial Clinical status ABPI Symptom free 1 or more Intermittent claudication 0.95 - 0.5 Rest pain 0.5 - 0.3 Gangrene and ulceration <0.2 |
| Drug treatment to reduce withdrawal symptoms in smoking | Nicotine replacement therapy Bupropion - reuptake inhibitor of dopamine, norepinephrine and serotonin varenicline - competitive inhibitor of nicotine, a partial agonist also, eases withdrawal symptoms |
| Pink frothy cough? | pulmonary oedema seconday to heart failure |
| Pleuritic pain is more common with broncho or lobar pneumonia | Lobar pneumonia |
| Common and rarer causes of haemoptysis | Common - acute bronchitis, TB Rarer - bronchiectasis, lobar pneumonia |
| Smokers cancer cell type | squamous |
| Pulmonary oedema vs idiopathic pulmonary fibrosis crackles | Pulmonary oedema - fine and at end of inspiration Idiopathic pulmonary fibrosis - coarser and heard earlier in inspiration |
| Pleural fluid exudate | Protein >30g/l, lactic dehydrogenase >200 IU/L |
| How to grade COPD | FEV1 as a percentage of expected for age/sex/height Mild 80%, Moderate 50-79%, severe 30-49%, very severe <30% |
| What is pneumoconiosis | Group of lung diseases caused by inhalation and retention of dust in the lung. causes a range of granulomatous and fibrotic change. Asbestosis is an example |
| What is allergic fibrosing alveolitis | antigen-antibody reaction (type III). Chronic exposure eventually leads to granulomas and chronic interstitial pneumonitis |
| Drugs not recommended in pulmonary hypertension and cor pulmonale | ACEi CCBs Alpha blockers Digoxin (unless there is AF) |
| Magic number for home o2 consideration | <7.3 kpa or < 8 with certain morbidities |
| Notable blood results in PE | Polymorphonuclear leucocytosis Elevated ESR increased lactate dehydrogenase |
| When to suspect empyema in pneumonia | fever and leukocytosis after 4-5 days of abs |
| Common causes of transudate | heart failure cirrhosis hypoalbuminaemia peritoneal dialysis |
| how to investigate suspected DVT | Ultrasound and if result negative then a D-dimer test Repeat test 6-8 days later in |
| What do the following tests assess RAST Prick test Patch test | RAST and Prick - type 1 hypersensitivity Patch test - delayed hypersensitivity |
| Derm, two types of herpes simplex virus | Type 1 - usually facial or non genital Type 2 - commonly genital, although distinction is not absolute |
| How to treat genital herpes | oral famciclovir or valaciclovir |
| Chicken pox timing | viral replication in lymph nodes over 2-4 days 4-6 days later a primary viraemia after a week a secondary viraemia to the viscera and skin eliciting the typical lesions New lesions erupt for 4-5 days fever usually 2-3 days from 38.5 to 40 |
| Pharm management of fungal infections | Terbinafide 250 daily or itraconazole 100mg daily |
| Problems with turbinated and keotconazole | hepatotoxicity |
| Drugs that can exacerbate psoriasis | NSAIDs, ACEi, lithium, chloroquine |
| 4 main varieties of melanoma | Superficial spreading Lentigo Acral lentiginous Nodular |
| Melanoma staging Tis to T4 | Tis - very top layer T1 - 1mm thick T2 - between 1-2mm thick T3 - between 2 and 4 mm thick T4 - melanoma more than 4mm thick |
| How to diagnose type 1 and type 4 hypersensitivity reactions | Type 1 - rast and skin prick tests Type 4 - patch testing |
| systemic treatments in eczema | Tetracyclines such as oxytetracycline, lymecycline Isotretinoin |
| Problems in Gorlins syndrome | Multiple BCC, jaw cysts, palmoplantar cutaneous pits, skeletal abnormalities |
| Topical options for actinic keratosis | 3% diclofenac gel (solaraze) Fluorouracil (efudix, actikerall) Ingenol mebutate |
| ABCD of melanoma | Asymmetry Irregular border Irregular colour Diameter >1cm Also inflammation, itch, bleeding or weeping |
| Diagnosis and initial management of asthma in children | |
| Obstructive and restrictive lung diseases and their FEV1/FVC | Obstructive - FEV1/FVC <0.7 -COPD, asthma, bronchiectasis, CF Restrictive - FEV1/FVC >0.7 -fibrosis, Sarcoidoisis, pneumoconiosis, interstitial pneumonia, connective tissue disorders, pleural effusion, obesity; kyphoscoliosis, neuromuscular problems, ARDS, Amiodarone, methotrexate |
| Investigation of Asthma in adults and initial management | |
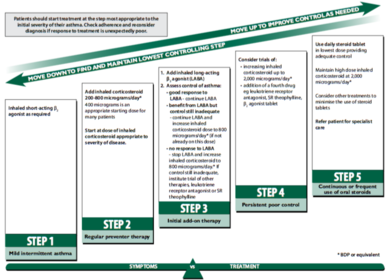
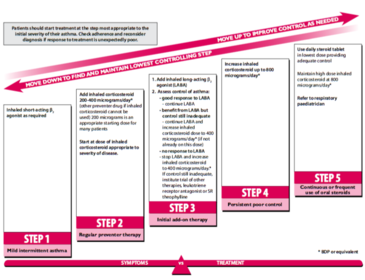
| Management of asthma in adults 12 years and up | |
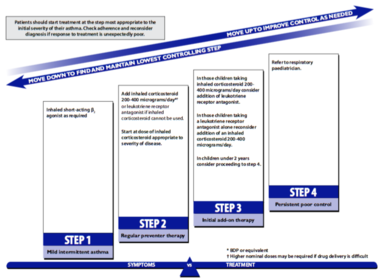
| Management of Asthma in 5-12 years old | |
| Management of asthma in under 5 years old | |
| Non-pharmacological management of asthma | Stop smoking Weight loss Breathing exercise programmes (can be physic taught) |
| What is this: most commonly affects trunk patches may be hypopigmented, pink or brown scale is common mild pruritus | Pityriasis versicolor, also called tinea versicolor, is a superficial cutaneous fungal infection caused by Malassezia furfur (formerly termed Pityrosporum ovale) patches may be hypopigmented, pink or brown (hence versicolor) |
| Management of heart failure | NICE issued updated guidelines on management in 2010, key points include: first-line treatment for all patients is both an ACE-inhibitor and a beta-blocker second-line treatment is now either an aldosterone antagonist, angiotensin II receptor blocker or a hydralazine in combination with a nitrate if symptoms persist cardiac resynchronisation therapy or digoxin* should be considered diuretics should be given for fluid overload offer annual influenza vaccine offer one-off** pneumococcal vaccine |
| Main indications for chest drain in pleural infections | Patients with frankly purulent or turbid/cloudy pleural fluid on sampling should receive prompt pleural space chest tube drainage. The presence of organisms identified by Gram stain and/or culture from a non-purulent pleural fluid sample indicates that pleural infection is established and should lead to prompt chest tube drainage. Pleural fluid pH < 7.2 in patients with suspected pleural infection indicates a need for chest tube drainage. |
| What to do about a pneumothorax | Primary pneumothorax Recommendations include: if the rim of air is < 2cm and the patient is not short of breath then discharge should be considered otherwise aspiration should be attempted if this fails (defined as > 2 cm or still short of breath) then a chest drain should be inserted patients should be advised to avoid smoking to reduce the risk of further episodes - the lifetime risk of developing a pneumothorax in healthy smoking men is around 10% compared with around 0.1% in non-smoking men Secondary pneumothorax Recommendations include: if the patient is > 50 years old and the rim of air is > 2cm and/or the patient is short of breath then a chest drain should be inserted. otherwise aspiration should be attempted if the rim of air is between 1-2cm. If aspiration fails (i.e. pneumothorax is still greater then 1cm) a chest drain should be inserted. All patients should be admitted for at least 24 hours if the pneumothorax is less the 1cm then the BTS guidelines suggest giving oxygen and admitting for 24 hours avoid diving |
| When to consider referral for familial hypercholesterolaemia | a total cholesterol concentration more than 7.5 mmol/litre and a family history of premature coronary heart disease. Refer anyway in people with - a total cholesterol concentration of more than 9.0 mmol/litre or a non‑HDL cholesterol concentration of more than 7.5 mmol/litre |
| secondary causes of dyslipidaemia to be excluded before specialist referral | excess alcohol, uncontrolled diabetes, hypothyroidism, liver disease and nephrotic syndrome |
| Bloods, assessments and management of which conditions in someone considered for dyslipidaemia | smoking status alcohol consumption blood pressure (see hypertension [NICE guideline CG127]) body mass index or other measure of obesity (see obesity [NICE guideline CG43]) total cholesterol, non‑HDL cholesterol, HDL cholesterol and triglycerides HbA1c renal function and eGFR transaminase level (alanine aminotransferase or aspartate aminotransferase) thyroid‑stimulating hormone. |
| Cholesterol goal in those started in statin | Measure total cholesterol, HDL cholesterol and non‑HDL cholesterol in all people who have been started on high‑intensity statin treatment at 3 months of treatment and aim for a greater than 40% reduction in non‑HDL cholesterol. If a greater than 40% reduction in non‑HDL cholesterol is not achieved: discuss adherence and timing of dose optimise adherence to diet and lifestyle measures consider increasing the dose if started on less than atorvastatin 80 mg and the person is judged to be at higher risk because of comorbidities, risk score or using clinical judgement Acceptable conservative LDL level ?4mmol/l |
| deep vs superficial venous ulcers | Deep venous insufficiency is related to previous DVT and superficial venous insufficiency is associated with varicose veins |
| When to start an inhaled corticosteroid | Inhaled steroids should be considered for patients with any of the following asthma-related features: exacerbations of asthma in the last two years using inhaled β2 agonists three times a week or more symptomatic three times a week or more waking one night a week |
| when to use an aldosterone antagonist in heart failure | patients who have had an acute MI and who have symptoms and/or signs of heart failure and left ventricular systolic dysfunction, treatment with an aldosterone antagonist licensed for post-MI treatment (e.g. eplerenone) should be initiated within 3-14 days of the MI, preferably after ACE inhibitor therapy |
| PCI window of opportunity | 90 minutes |
| thrombolysis window of opportunity | 12 hours |
| simple step up management for acne | single topical therapy (topical retinoids, benzyl peroxide) topical combination therapy (topical antibiotic, benzoyl peroxide, topical retinoid) oral antibiotics: e.g. Oxytetracycline, doxycycline. Improvement may not be seen for 3-4 months. Minocycline is now considered less appropriate due to the possibility of irreversible pigmentation. Gram negative folliculitis may occur as a complication of long-term antibiotic use - high-dose oral trimethoprim is effective if this occurs oral isotretinoin: only under specialist supervision |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.