427428
Description
Mind Map by greenfylde, updated more than 1 year ago
|
|
Created by greenfylde
over 10 years ago
|
|
Headache
Annotations:
- v common, usually benign
- Meningitis
- viral- usually self limiting, headache main feat
- bact- life threat: decreased GCS, shock signs, purpuric rash (non blanch), focal neuro signs
- beware atyp presentation: immunosuppressed, preg, alcoholic patients
- organisms
- meningococcus or pneumococcus
- less: H influenze; Listeria monocytogenes. If HIV +ve: CMV, cryuptococcus or TB if HIV +ve
- meningococcus or pneumococcus
- differential diag
- malaria
- encephalitis
- septicemia
- subarachnoid
- dengue
- tetanus
- malaria
- features
- classic triad: headache, fever, meningism (stiff neck, photophobia + headache)
- onset: hours
- early: headache, leg pains, cold hands and feeet, flu-ey abnormal skin color
- later: meningism: neck stiff + photophobia, Kernig's sign (pain and resistance on passive knee extension w/hip fully flexed)
- decreased conscious lvl, coma; seizures (20%) +/- focal CNS signs (20%) +/- opisthotonus; petechial rash (non-blanching - may only be 1 or 2 spots)
- signs of galloping sepsis: slow cap refil; DIC; BP down, Temp and pulse up or normal
- classic triad: headache, fever, meningism (stiff neck, photophobia + headache)
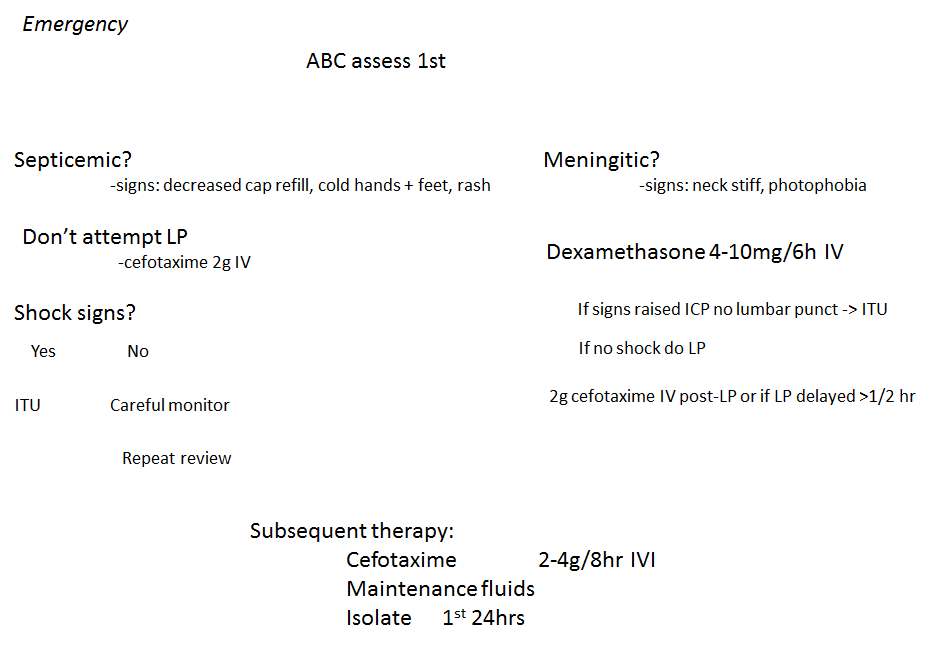
- treatment
- when to act now: if any 2 coexist, give
BENZYLPENICILLIN 1.2 IM/IV before admitting
if pt not yet in hosp
- headache
- raised temp
- neck stiffness
- altered mental state
- headache
- if raised ICP, summon help and inform neurosurg
- prophylaxis: household contacts in droplet range or those who have kissed pts mouth (rifampicin, ciprofloxin)
- antiobiotics stat (see trust guidelines eg cefotaxime or aciclovir if viral)
- when to act now: if any 2 coexist, give
BENZYLPENICILLIN 1.2 IM/IV before admitting
if pt not yet in hosp
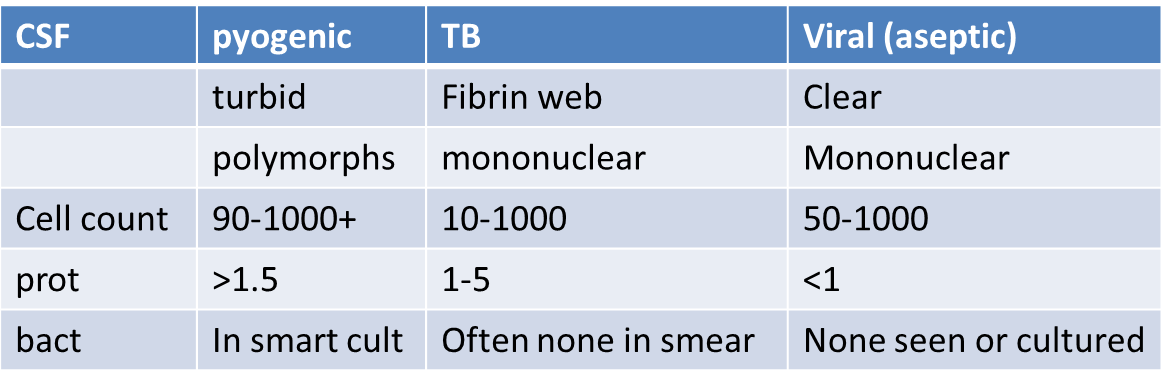
- investig
- LP- helpful, but don't delay IV antibiotics
- usually done after CT but safe w/o (if no mass or raised CIP suspected- look for papillodema, focal signs, decreased cons)
- for mets, gram stain, protein, glucose, virology/PCR, and lactate
- usually done after CT but safe w/o (if no mass or raised CIP suspected- look for papillodema, focal signs, decreased cons)
- U + E, FBC (WBC decreased- immunocomp) LFT, glucose, coag screen
- blood cult, throat swab, rectal swab for viruses. Serology eg EBV, HIV
- if aseptic meningitis (usually self limiting) do CSF PCR
- CXR (signs of TB? -> TB meningitis)
- LP- helpful, but don't delay IV antibiotics
- viral- usually self limiting, headache main feat
- Migraine
Annotations:
- migraines often co-exists w/other chornic probs treat person as whole -> aim = recover life
- recurrent severe
headaches lasting hrs-
few days (4-72 hours)
- common trigggers
Annotations:
- C-heese H-cHoc O-ral contracep C-affeine O L -alcohOL A-nxiety T-ravel E-xercise
- cheese, choc, alch, oral contracep
- 50% no trigger
- epidem
- first attack age >40 uncommon
- prevalence 8% F:M 2:1
- big cost £200million per year
- first attack age >40 uncommon
- symptoms
- usually +: photophobial, N + V
- intense, throbbing, unilat, favor bedrest in quiet+ dark
- visual or other aura lasting 15-30min
- followed by 1h unilat, THROBBING headache
- or isolated aura w/no headache
- or episodic severe headaches without aura,
often premenstrual usually unilat, with N+ V +/-
photophobia/phonophobia
- usually +: photophobial, N + V
- signs
- none
- (so PERFECT FOR OSCE)
- none
- assocs
- obesity
- patent foramen ovale
- obesity
- tests
- NONE if typical hx
- NONE if typical hx
- prodrome (maybe hrs or days)
- yawning, food cravings or changes in sleep, appetite, mood
- yawning, food cravings or changes in sleep, appetite, mood
- aura
- precedes by mins + may persist during
- visual- chaotic cascading, distorting,
'melting' and jumbling of lines, sigzags,
scotomata, hemianopia
- somatosensory- paresthesiae fingers -> face
- motor: dysarthria + ataxia (basilar migraine); opthalmoplegia or hemiparesis
- speech (8% of auras); dysphaia or paraphasia (eg phoneme substitution)
- precedes by mins + may persist during
- Diag criteria if no aura
- 5+ lasting 4-72 hrs w/1 of : N+ V or phto/phonophobia and 2+ of: unilat,
pulsating, interferes w/normal life, worsened by routine activity (eg stairs)
- 5+ lasting 4-72 hrs w/1 of : N+ V or phto/phonophobia and 2+ of: unilat,
pulsating, interferes w/normal life, worsened by routine activity (eg stairs)
- differential
Annotations:
- cluster tension cervical spondylosis increased BP intracranial pathology sinusitis/otitis media caries TIAs may mimic migraine aura. migraine rarely sign of other pathology
- extra notes for F
Annotations:
- -perimenstural migraine: do NSAID at onset of menses to last day of bleeding +/- transdermal estradiol for 7 days starting 3d before menses -preg :migraine often better. if not, may have increased risk of pre-eclampsia and CVS complics -DON'T GIVE COCONTRACEP if migraines, partic if aura b/c increased risk of stroke
- treatment
- NSAIDs (less chance of med misuse headache)
Annotations:
- eg ketoprofen 100 mg dispersible aspirin 900mg/6h
- triptans
Annotations:
- 5HT IB/ID agonists- constrict cranial arts rizatriptan, sumatriptan NOT if IHD, coronary spasm, uncontrolled hypertension, recent lithium, SSRIs or ergot use
- ergotamine
Annotations:
- 1mg PO as headache starts, repeated at 1/2 hr
- prophylaxis if freq >2x/mo
Annotations:
- most achieve 50% decrease in attack frequency
- propranolol, topiramate, amitryptilline
Annotations:
- 2nd line: valproate, pizotifen, gabapentin, pregerbalin, or NSAIDS
- non pharm treat
Annotations:
- warm or cold packs to head rebreath into paper bag spinal manip, riboflavin, magnesium
- NSAIDs (less chance of med misuse headache)
- Tension/Stress Headache
- usually bilat (often generalised or frontal)
- 'dull' 'tight' 'pressing', non pulsatile; +/- scalp musc tender
- N + V usually ABSENT
- pt can continue w/normal activities
- recurrent
- NO neuro signs
- treatment
- stress relief + massage
Annotations:
- may help more than neurology
- reassurance; avoid triggers
- antidepressants
- analgesia
- stress relief + massage
- usually bilat (often generalised or frontal)
- sub-arachnoid
hemorrhage
Annotations:
- spontaneous bleeding into subarach space -often catastrophic
- epidem
- typically 35-65
- annual incidence 9/100,000
- risk facotrs
- smoking, alcohol misuse, hypertension,
bleeding disorders, FH, mycotic aneurysm (SBE),
perhaps post-menopausal decrease
estrogen? (F:M 3:2 once >45y)
- smoking, alcohol misuse, hypertension,
bleeding disorders, FH, mycotic aneurysm (SBE),
perhaps post-menopausal decrease
estrogen? (F:M 3:2 once >45y)
- typically 35-65
- causes
- 80% rupture of saccular (berry) aneurysm
Annotations:
- common sites for berry aneurysm: junction of post communic w/internal carotid OR junct of ant communic w/ant cerebral artery or bifurc of middle cerebral art 15% are multiple assocs: polycystic kidnesy, coarct of aorta, Ehlers Danlos synd
- arteriovenous malformations (15%)
- 80% rupture of saccular (berry) aneurysm
- clin feats
- symps
- sudden onset (seconds), severe, occipital
- 'though i'd been kicked in head'
- 'though i'd been kicked in head'
- vomiting, collapse, seizures + coma often follow
- coma/drowsiness may last for days
- coma/drowsiness may last for days
- sudden onset (seconds), severe, occipital
- signs
- distress and photophobia common, but
nect stiff may take hrs to devel
- kernig's sign (takes 6h to devel)
Annotations:
- each hip flxed in turn, then try to straighten knee while hip flexed in meningitis, this move gretly limited by spasm of hamstrings
- focal neurology at presentation may suggest site
Annotations:
- of aneurysm (eg pupil changes indicating a IIIrd nerve palsy w/a posterior communicating artery aneurysm or intracerebral hematoma later deficits suggest complics
- sentinel headache
Annotations:
- may have had small warning leak from aneurysm (6%) be suspiciuos of ANY sudden headache w/neck or back pain (surg is more successful in the least symptomatic)
- distress and photophobia common, but
nect stiff may take hrs to devel
- symps
- differential
Annotations:
- in py care only 25% of thunderclap headache is SAH in50-65% no cause found remainder -> meningitis, migraine, intracerebral bleeds, cortical vein thrombosis
- benign thunderclap headache mimicks SAH but investig shows no evidence of intravasc disord
- investigs
- CT w/in 48hrs(>90% evident- if not do LP- for yellow sign)
- LP if CT -ve and no contraindic >12hr after headache onset
- CSF
- uniformly bloody early on
- becomes XANTHOCHROMIC (yellow) after several hrs to to Hb breakdown. confirms SAH b/c not just a blood tap
- uniformly bloody early on
- CT w/in 48hrs(>90% evident- if not do LP- for yellow sign)
- management
Annotations:
- prognosis no signs- 0% neck stiff + CN palsy- 11% mort drowsy- 37% drowsy w/hemiplegia 71% prolonged coma- 100% in 1st mo
- all proven SAH -> refer to neurosurg immediately
- re-examine CNS often
Annotations:
- chart BP, pupils, GCS, repeat CT if deteriorating
- maintain cereb perfusion by keep well hydrated
Annotations:
- aim for SBP >160mmHg treat high BP only if very severe
- nimodipine
Annotations:
- for 3w Ca2+ antag that decreases vasospasm + consequent morbidity from cerebral ischemia
- endovascular coiling
Annotations:
- preferable to surgical clipping do CT angiography or catheter to ID single vs multiple aneurysms prior to intervention intracranial stents and balloon remodelling for wide necked aneruysms
- complics
- large bleed? may be complic by decreased GCH, seizure or focal neuro signs
- REBLEEDING
Annotations:
- often in 1st few days. occurs in 20%. Is commonest Cause of Death
- CERBRAL ISCHEMIA due to vasospasm
Annotations:
- commonest cause of morbidity. may cause permanent CNS deficit
- hydrocephalus- requires drain
- hyponatremia
Annotations:
- common but should not be managed w/fluid restriction. seek expert help
- large bleed? may be complic by decreased GCH, seizure or focal neuro signs
- giant cell arteritis
Annotations:
- aka temporal arteritis
- large vess vasculitis
- close assoc w/PMR (polymyalgia rheumatica)
- F>M, unusual if <50
- exclude in all >50yrs w/a headache that has lasted a few weeks
- exclude in all >50yrs w/a headache that has lasted a few weeks
- clin feats
- localised temporal/occipital headache
- scalp tender
- jaw claudic
- sudden onset visual loss
- prompt daig + steroids avoid blindness
- prompt daig + steroids avoid blindness
- thickened, tender, PULSELESS temporal arts
- ESR >40mm/h
- extracranial symps
- constitutional upset (malaise, night sweats, pyrexia, weight loss)
- dyspnea, morning stiff, unequal or weak pulses
- constitutional upset (malaise, night sweats, pyrexia, weight loss)
- localised temporal/occipital headache
- treat
- treat urgently with steroids
Annotations:
- because potential RAPID ONSET VISUAL LOSS
- (if suspect GCA, do ESR and give
steroids (prenisolone) immediately
- temproal art biopsy (get w/in 3 days of starting steroids) may confirm, but don't delay treat
Annotations:
- skip lesions occur -so don't be put off by neg biopsy
- treat urgently with steroids
- investigs
- ESR + CRP ++
- platelets +
- alk phos +
- Hb -
- ESR + CRP ++
- prognosis
Annotations:
- typically 2 year course, then complete remission reduce prednisolone after 5-7d guided by symps + ESR increase dose if symps recur main COD + morbidity is long term steroid treat give gastric + bone protect (PPI and alendronic acid)
- stroke
- sinusitis
- dull throbbing headache, assoc w/facial pain over sinuses
- worse on bending forward
- ALWAYS NASAL SYMPS eg congest or discharge
- if ?8w req CT to confirm diag
- dull throbbing headache, assoc w/facial pain over sinuses
- other vasc cuases
- intracerebellar hemorrahge
Annotations:
- -abrupt onset headache -N and v -dizzy -ataxia +/- GCS
- Spontaneous intracerebral or intraventricular hemorrhage
Annotations:
- onset min -> hrs. accompany by focal neuro deficit +/- GCS
- Cerebral venous thrombosis
Annotations:
- headache common but variable 'thunderclap' throbbing 'band-like' (may have assoc feats- eg N and V, seizures, CN palsies, hemiparesis, ataxia, decreased GCS)
- Vertebrobasilar dissection
Annotations:
- maybe acute occipital/post neck pain with brainstem signs/symps
- intracerebellar hemorrahge
- other
- cluster
- severe, unilat
- retroorbital
- 5+ episodes
- agitation, restlessness, ipsilat lacrimation, conjunctival injection, rhinorrhea, facial sweating
- attacks short (15-90min) but frequent (1 per 2 days -> 8 per day)
- repeated, ( often same time each day), in clusters (days -> wks) separated by months w/o symps
- agitation, restlessness, ipsilat lacrimation, conjunctival injection, rhinorrhea, facial sweating
- M: F 5: 1
- severe, unilat
- acute glaucoma
- because sudden increase ocular pressure
- typical pt
- long sighted, middle age/elderly
- long sighted, middle age/elderly
- present
- periorbital plain
- N + V
- blurred vision with halos aroudn lights + conjunctival injection
- periorbital plain
- urgent opthalmology referral mandatory
- because sudden increase ocular pressure
- raised ICP
- maybe primary (idiopathic)
- espec in overweight young females on oral contracep
- espec in overweight young females on oral contracep
- or secondary to Space Occupying Lesion
- clin signs
- focal neuro signs
- change in personality
- new-onset seizures
- headache, wosre in morning, lying flat, coughing or straining
- assoc? vomiting (often w/o nausea +/- papilloedema)
- focal neuro signs
- clin signs
- maybe primary (idiopathic)
- other
- cluster
- TMJ syndromes
- drugs
- analgesic headache
- assoc chronic analgesic use
espec opioid eg codeine
- usualy bilat
- occur prior to next dose of analgesia
- assoc chronic analgesic use
espec opioid eg codeine
- vasodilats eg nitrates
- rec drugs eg solvents
- analgesic headache
- RED FLAG FEATS
- new onset headache/change in headache (pt over 50)
- focal CNS signs, ataxia, or new cognitive or behavioural disturbance
- persistent visual disturb
- headache that changes w/posture or wakes pt up
- headache brough on by physical exertion
- papilledema
- new onset headache in pt w/known HIV or active malig
- new onset headache/change in headache (pt over 50)
Media attachments
{kind=link}
{kind=link}
Want to create your own Mind Maps for free with GoConqr? Learn more.