4807785
Description
Mind Map by Charlotte Summerly, updated more than 1 year ago
|
|
Created by Charlotte Summerly
almost 10 years ago
|
|
Psychopathology
- Mental
Disorders
- Phobias
- Emotional - excessive and unreasonable which is
coupled with anxiety and panic. Cued by the presence of
anticipation of the object or situation
- Behavioural - Avoidance, freeze or faint, . It interferes
with the person's normal routine.
- Cognitive - irrational thinking and resistance to rational
arguments. Recognises that the fear is excessive or
unreasonable.
- Emotional - excessive and unreasonable which is
coupled with anxiety and panic. Cued by the presence of
anticipation of the object or situation
- Depression
- Emotional - sadness, loss of interest, low self esteem and
anger due to lack of control
- Behavioural - increase/decrease in activity levels,
insomnia, poor appetite
- Cognitive - negative emotions and thoughts, irrational
thoughts
- Emotional - sadness, loss of interest, low self esteem and
anger due to lack of control
- OCD
- Emotional - anxiety and stress, feelings
of embarrassment, disgust
- Behavioural - repetitive and concealed to perform
these actions
- Cognitive - seen as uncontrollable, recurrent
and intrusive thoughts
- Emotional - anxiety and stress, feelings
of embarrassment, disgust
- Phobias
- Definitions of
abnormality
- Statistical Infrequency
- If the behaviours reach either end of the scale it is
normally seen as abnormal, however, some may be
good
- Abnormality is defined as those behaviours that are extremely
rare
- I; Abnormal can be seen as desirable. J; High IQ could still be seen as desirable.
E; Identification between desirable and undesirable has to be found
- I; Can be appropriate to use a statistical criterion. J; Can be used for the cut off of
abnormality . Two SD or below it is seen as abnormal. E; Shows statistical
infrequency may be inappropriate
- I; Can be appropriate to use a statistical criterion. J; Can be used for the cut off of
abnormality . Two SD or below it is seen as abnormal. E; Shows statistical
infrequency may be inappropriate
- If the behaviours reach either end of the scale it is
normally seen as abnormal, however, some may be
good
- Deviation from social norms
- Abnormal behaviour is seen as deviant from
unstated rules about how one 'ought' to behave.
Anything that violates these rules are seen as
abnormal
- Rules are based around
explicit rules (laws) and
implicit rules (personal
beliefs made by culture)
- An example is homosexuality - once
seen as abnormal and were put into
mental institutions but now it is
seen as a social norm
- An example is homosexuality - once
seen as abnormal and were put into
mental institutions but now it is
seen as a social norm
- Rules are based around
explicit rules (laws) and
implicit rules (personal
beliefs made by culture)
- I; Main difficulty is that it
varies as times change. J;
E.g homosexuality was once
seen as abnormal but now
it is a social norm. E; Shows
that social morals and
attitudes can change
- I; Making judgements on deviance is often related to context of
behaviour. J; Many cases there is not a clear line between what is
abnormal and what is eccentric. E; Means that social deviance cannot
make a complete definition for abnormality as it relies on context
- I; Making judgements on deviance is often related to context of
behaviour. J; Many cases there is not a clear line between what is
abnormal and what is eccentric. E; Means that social deviance cannot
make a complete definition for abnormality as it relies on context
- Abnormal behaviour is seen as deviant from
unstated rules about how one 'ought' to behave.
Anything that violates these rules are seen as
abnormal
- Failure to Function Adequately
- People are judges on their ability to go
about daily life.
- Could be a situation where the individual is not having
any distress but it could be causing distress for others
- The DSM and WHODAS - includes understanding and
communicating, self care and life activities
- I; Recognises the subjective experience of patients.
J; It is relatively easy to judge objectively as we can
list behaviours. E; Shows strengths
- I; Someone needs to decide if it actually the
case. J; Could be that individual is content but it
is that others are uncomfortable and
behaviours are abnormal. E; Weakness is that it
depends on who is making the judgement
- I; Someone needs to decide if it actually the
case. J; Could be that individual is content but it
is that others are uncomfortable and
behaviours are abnormal. E; Weakness is that it
depends on who is making the judgement
- I; Recognises the subjective experience of patients.
J; It is relatively easy to judge objectively as we can
list behaviours. E; Shows strengths
- The DSM and WHODAS - includes understanding and
communicating, self care and life activities
- Could be a situation where the individual is not having
any distress but it could be causing distress for others
- People are judges on their ability to go
about daily life.
- Deviation from social norms
- Jahoda conducted PRAISE - Personal
growth, reality perception, autonomy,
integration, self attitudes and
environmental mastery.
- Absence of this can suggest possible
mental disorders and abnormality
- I; Has an unrealistic criteria. J; Jahoda
presents an ideal criteria but it could be
difficult to assess specific criteria. E; Not
really useable when comes to
abnormality
- I; Mental health is same as physical
health. J; Physical is easy to detect
whereas mental health is normally a
consequence from life experiences. E;
Unlikely that mental abnormality is
diagnosed is same as physical health.
- I; Mental health is same as physical
health. J; Physical is easy to detect
whereas mental health is normally a
consequence from life experiences. E;
Unlikely that mental abnormality is
diagnosed is same as physical health.
- I; Has an unrealistic criteria. J; Jahoda
presents an ideal criteria but it could be
difficult to assess specific criteria. E; Not
really useable when comes to
abnormality
- Absence of this can suggest possible
mental disorders and abnormality
- Jahoda conducted PRAISE - Personal
growth, reality perception, autonomy,
integration, self attitudes and
environmental mastery.
- Statistical Infrequency
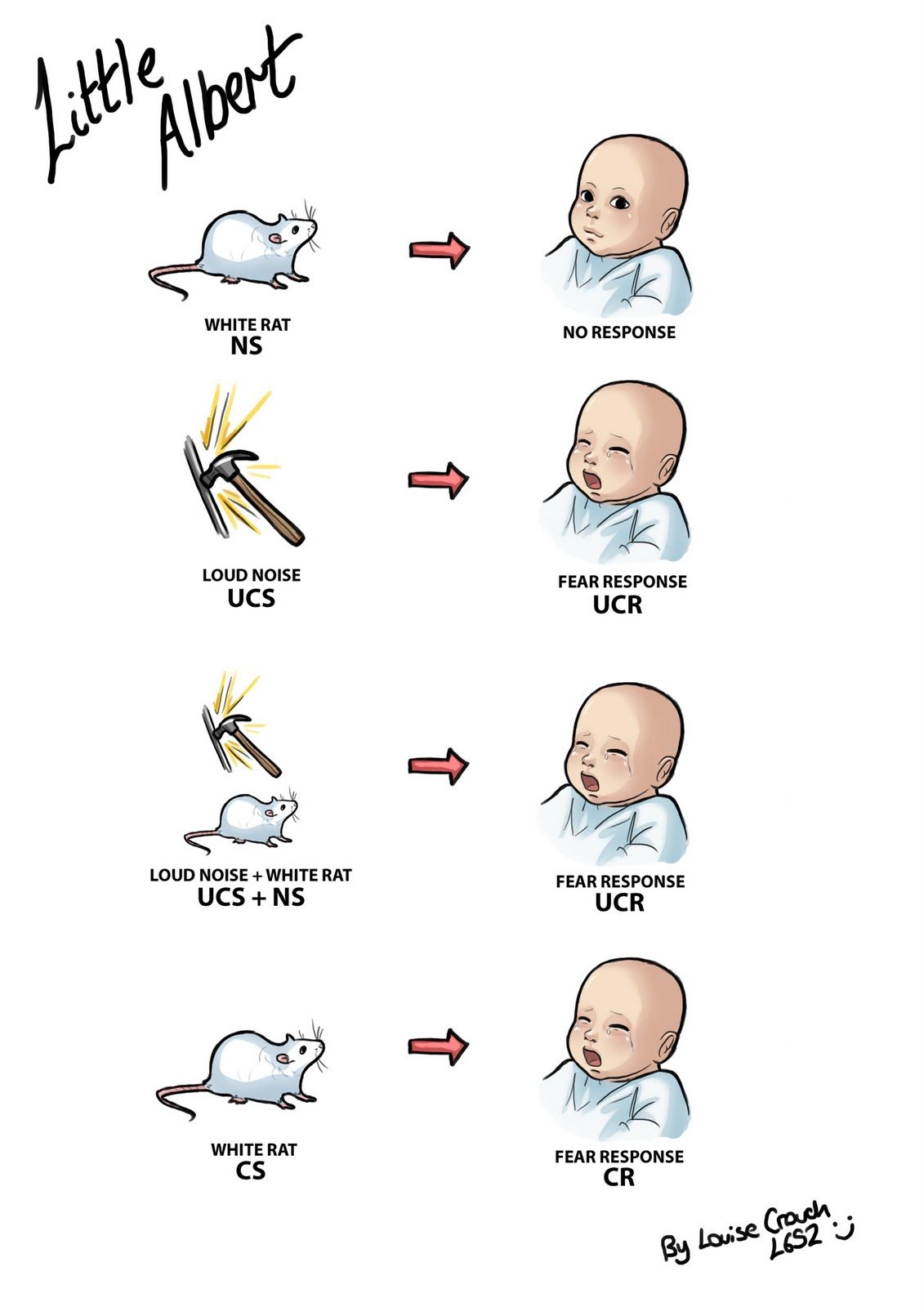
- Behavioural Approach -
Explaining Phobias
- Operant conditioning - avoidance of
the phobic stimulus reduces fear and
is this reinforcing. This is an example
of negative reinforcement. Reward is
them not having anxiety
- Phobias
may also
be
acquired
through
modelling
behaviour
of others
- I; Some support for CC. J; Often able to recall when a phobia
occurred e.g. being bitten by a dog. E; However, not everyone
can do this because the situation has been forgotten.
- I; Could be explained by diathesis stress
model. J; Individual has genetic
vulnerability for developing a mental
disorder. E; However, will only occur if
there has been a trigger.
- I; Phobias don't always develop after a traumatic
incident - biological preparedness. J; Animals are
scared of ancient fears that would be dangerous
in evolutionary past. E; Explains why we are less
likely to develop fears of modern objects
- I; Phobias don't always develop after a traumatic
incident - biological preparedness. J; Animals are
scared of ancient fears that would be dangerous
in evolutionary past. E; Explains why we are less
likely to develop fears of modern objects
- I; Could be explained by diathesis stress
model. J; Individual has genetic
vulnerability for developing a mental
disorder. E; However, will only occur if
there has been a trigger.
- Phobias
may also
be
acquired
through
modelling
behaviour
of others
- Operant conditioning - avoidance of
the phobic stimulus reduces fear and
is this reinforcing. This is an example
of negative reinforcement. Reward is
them not having anxiety
- Behavioural Approach -
Treating Phobias
- Flooding
- Patient experiences their phobia at
its worst whilst using relaxation.
Finished in one long session.
Adrenaline levels decrease, a new
association can be made
- I; Individual differences. J;
Flooding is not for every patient
as it could be traumatic for
them. E; They may still wait and
therapy will not be as effective.
- I; Appears flooding can be
effective and relatively quick. J;
Researchers said both treatments
were good but flooding is more
effective. E; However, others say
both treatments are effective
- I; Appears flooding can be
effective and relatively quick. J;
Researchers said both treatments
were good but flooding is more
effective. E; However, others say
both treatments are effective
- I; Individual differences. J;
Flooding is not for every patient
as it could be traumatic for
them. E; They may still wait and
therapy will not be as effective.
- Patient experiences their phobia at
its worst whilst using relaxation.
Finished in one long session.
Adrenaline levels decrease, a new
association can be made
- Systematic Desensitation
- Counter Conditioning - patient is taught a
new association that runs counter to the
original association
- Relaxation - therapist teaches client new
relaxation techniques e.g. slow breathing
- Desensitisation Hierarchy - works by
gradually introducing patient to feared
situation one step at a time
- Step 1 - relax muscles. Step 2 -
contrast hierarchy of scenes.
Step 3 - patient works through
hierarchy. Step 4 - Patient
mastered one step and moves
to next. Step 5 - patient
eventually mastered the fear
- I; Found SD is successful of phobias. J; 75%
patients respond to SD and actual contact
is most beneficial with stimulus E; Shows
there is some effectiveness with SD.
- I; Generally relatively fast and requires less effort on
patients part. J; E.g - CBT requires lot of willpower from
patient to understand. E; Lack of thinking is useful for
people with lack of insight into motivations.
- I; Generally relatively fast and requires less effort on
patients part. J; E.g - CBT requires lot of willpower from
patient to understand. E; Lack of thinking is useful for
people with lack of insight into motivations.
- I; Found SD is successful of phobias. J; 75%
patients respond to SD and actual contact
is most beneficial with stimulus E; Shows
there is some effectiveness with SD.
- Step 1 - relax muscles. Step 2 -
contrast hierarchy of scenes.
Step 3 - patient works through
hierarchy. Step 4 - Patient
mastered one step and moves
to next. Step 5 - patient
eventually mastered the fear
- Desensitisation Hierarchy - works by
gradually introducing patient to feared
situation one step at a time
- Relaxation - therapist teaches client new
relaxation techniques e.g. slow breathing
- Counter Conditioning - patient is taught a
new association that runs counter to the
original association
- Flooding
- Cognitive Approach -
Explaining
Depression
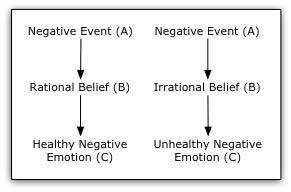
- Mustabatory Thinking -
thinking that certain
ideas or assumptions
must be true in order for
an individual to be happy
- An individual who holds
these is likely to be
disappointed or at worst
depressed
- An individual who holds
these is likely to be
disappointed or at worst
depressed
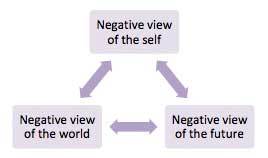
- Negative schema - likely that
depressed people have
developed a negative schema in
childhood, this could be caused
by factors such as peers. Biased
towards negative
interpretations and lack of
control
- I; Depression is linked with
irrational behaviour. J;
Hammen and Krantz found
depressed p's made more
errors in logic when asked to
interpret written material. E;
However, doesn't mean that
negative thoughts cause
depression
- I; Blames client for behaviour. J; Gives
clients power to change their ways. E;
However, may lead to client/therapist
to overlook situational factors
- I; Led to practical
applications in therapy. J;
Both models have been
applied to CBT as it found
to be best treatment for
depression. E; If
depression is alleviated
then it suggests that
irrational thinking has a
role in depression.
- I; Led to practical
applications in therapy. J;
Both models have been
applied to CBT as it found
to be best treatment for
depression. E; If
depression is alleviated
then it suggests that
irrational thinking has a
role in depression.
- I; Blames client for behaviour. J; Gives
clients power to change their ways. E;
However, may lead to client/therapist
to overlook situational factors
- Mustabatory Thinking -
thinking that certain
ideas or assumptions
must be true in order for
an individual to be happy
- Cognitive Approach -
Treating Depression
- CBT - combination of cognitive
and behavioural therapy to turn
irrational thoughts into rational
ones (REBT)
- Ellis extended ABC to ABCDEF -
disputing thoughts, effects of disputing
and feelings. Logical disputing,
empirical disputing and pragmatic
disputing
- Clients are often asked to
complete assignments to
challenge and test the irrational
beliefs that they believe in
- CBT involves specific
focus on encouraging
depressed clients to
become more active.
Therapists and client can
identify pleasurable
activities and deal with
cognitive barriers
- CBT involves specific
focus on encouraging
depressed clients to
become more active.
Therapists and client can
identify pleasurable
activities and deal with
cognitive barriers
- Clients are often asked to
complete assignments to
challenge and test the irrational
beliefs that they believe in
- Ellis extended ABC to ABCDEF -
disputing thoughts, effects of disputing
and feelings. Logical disputing,
empirical disputing and pragmatic
disputing
- I; Research to support
CBT. J; Ellis claimed
90% success rates, on
average 27 sessions
to complete. E;
However, may not be
as effective as beliefs
aren't put into action.
- I; CBT may be less suitable
to people with high
irrational beliefs. J; Found a
possible lack of success for
suitability as direct advice
is not always taken. E;
Shows individual
differences
- I; Alleviate depression
through exercise. J;
Major depressive
disorder - end of 6
months exercise group
had lower relapse rates
than medication groups.
E; Shows some support
for behavioural
activation
- I; Alleviate depression
through exercise. J;
Major depressive
disorder - end of 6
months exercise group
had lower relapse rates
than medication groups.
E; Shows some support
for behavioural
activation
- I; CBT may be less suitable
to people with high
irrational beliefs. J; Found a
possible lack of success for
suitability as direct advice
is not always taken. E;
Shows individual
differences
- CBT - combination of cognitive
and behavioural therapy to turn
irrational thoughts into rational
ones (REBT)
- Biological Approach -
Explaining Depression
- COMT Gene; involved in
the production of COMT,
regulates the production
of the neurotransmitter
dopamine that has been
implicated in OCD, one
form of the gene has been
found to be common in
OCD, produces lower
activity of COMT gene and
higher levels of dopamine
- SERT Gene; affects the transport of
serotonin, creating low levels of this
neurotransmitter. One study found
a mutation of this gene in two
unrelated families where 6/7 had
OCD.
- Diathesis-stress model; genes are implicated in a
number of disorders such as depression and post
traumatic stress disorder, it suggests that each
individual gene creates vulnerability for OCD. Other
factors (stressors) affect what the condition developed
but some may possess the gene but not suffer any
illness as there is no trigger
- Diathesis-stress model; genes are implicated in a
number of disorders such as depression and post
traumatic stress disorder, it suggests that each
individual gene creates vulnerability for OCD. Other
factors (stressors) affect what the condition developed
but some may possess the gene but not suffer any
illness as there is no trigger
- SERT Gene; affects the transport of
serotonin, creating low levels of this
neurotransmitter. One study found
a mutation of this gene in two
unrelated families where 6/7 had
OCD.
- Abnormal levels of
neurotransmitters; dopamine
levels are thought to be
abnormally high in people with
OCD, lower levels of serotonin
associated with OCD,
antidepressants increase
serotonin levels and reduce
symptoms OCD.
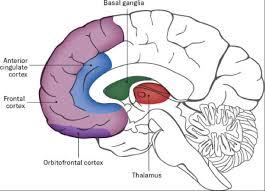
- Abnormal brain circuits;
caudate nucleus - signals from
OFC - signals to thalamus.
When nucleus is damaged -
thalamus is alerted - signals
back to OFC = WORRY CIRCUIT.
Supported from PET scans,
serotonin plays key role in OCD.
- Abnormal brain circuits;
caudate nucleus - signals from
OFC - signals to thalamus.
When nucleus is damaged -
thalamus is alerted - signals
back to OFC = WORRY CIRCUIT.
Supported from PET scans,
serotonin plays key role in OCD.
- I; There have been twin studies to show evidence for
the biological approach. J; A meta analysis on OCD
found that identical twins were more than twice as
likely to develop OCD if their co-twin did. E; However,
concordance rates are not 100% as some
environmental factors must have a role also
- I; There has been research
for Tourette's syndrome
and disorders. J;
Researchers found that OCD
is one form of expression if
the same gene that
determines Tourettes and
was also found the same
gene that determines
Tourettes and was also
found that both symptoms
are in autistic children.
- I; There has been
research to support
OFC and genes. J;
Researchers used MRI
to find brain activity in
OCD patients, families
without OCD and
unrelated people
finding that OCD does
affect the OFC. E; This
supports the view that
differences may lead to
OCD in individuals.
- I; There has been
research to support
OFC and genes. J;
Researchers used MRI
to find brain activity in
OCD patients, families
without OCD and
unrelated people
finding that OCD does
affect the OFC. E; This
supports the view that
differences may lead to
OCD in individuals.
- I; There has been research
for Tourette's syndrome
and disorders. J;
Researchers found that OCD
is one form of expression if
the same gene that
determines Tourettes and
was also found the same
gene that determines
Tourettes and was also
found that both symptoms
are in autistic children.
- COMT Gene; involved in
the production of COMT,
regulates the production
of the neurotransmitter
dopamine that has been
implicated in OCD, one
form of the gene has been
found to be common in
OCD, produces lower
activity of COMT gene and
higher levels of dopamine
- Biological Approach -
Treating OCD
- SSRIs; block the re-uptake of serotonin at
the presynaptic membrane, increasing
serotonin concentration at receptor sites
on the post synaptic membrane. E.g Proza
to increase levels of neurotransmitter
serotonin to regulate mood and anxiety
- Tricyclics; block the transporter
mechanism that reabsorbs with serotonin
and noradrenaline. As a result, more of
these neurotransmitters are left in the
synapse, prolonging the activity. Due to
them having more side effects they are
used as a second line treatment for when
SSRI is not effective
- Anti-anxiety drugs; benzodiazepines are
commonly used to reduce anxiety e.g. Diazepam.
Slows down anxiety of CNS by increasing activity
of GABA. GABA is released from neutron as it
travels across the gap and locks onto one of the
rector sites. Increases the flow of chloride ions
and slowing down the neuron and CNS - relaxing
the patient
- GABA regulates excitement in the
central nervous system and acting as a
natural form of anxiety reducer
- GABA regulates excitement in the
central nervous system and acting as a
natural form of anxiety reducer
- Anti-anxiety drugs; benzodiazepines are
commonly used to reduce anxiety e.g. Diazepam.
Slows down anxiety of CNS by increasing activity
of GABA. GABA is released from neutron as it
travels across the gap and locks onto one of the
rector sites. Increases the flow of chloride ions
and slowing down the neuron and CNS - relaxing
the patient
- Tricyclics; block the transporter
mechanism that reabsorbs with serotonin
and noradrenaline. As a result, more of
these neurotransmitters are left in the
synapse, prolonging the activity. Due to
them having more side effects they are
used as a second line treatment for when
SSRI is not effective
- I; There is considerable evidence for the effectiveness of
drug treatments. J; Researchers found SSRIs were more
effective than placebos in reducing the symptoms of OCD
up to 3 months after treatment. E; However, as studies are
only a short duration there is only very little long term
data
- I; A strength is that drug therapies are preferred to other
treatments such as CBT. J; From the point of the health
service they are also cheaper as they require little
monitoring and are cheap compared to psychological
treatments. E; However, some patients may benefit from
the fact of just talking to a doctor during consultations as
it could help.
- I; There is a problem with side
effects of drug therapy. J;
Common side effects of SSRIs are
insomnia, headaches and nausea,
tricyclics show hallucinations and
Bzs may show aggression. E; This,
therefore shows that there are
side effects with drug therapy in
treating OCD
- I; There is a problem with side
effects of drug therapy. J;
Common side effects of SSRIs are
insomnia, headaches and nausea,
tricyclics show hallucinations and
Bzs may show aggression. E; This,
therefore shows that there are
side effects with drug therapy in
treating OCD
- I; A strength is that drug therapies are preferred to other
treatments such as CBT. J; From the point of the health
service they are also cheaper as they require little
monitoring and are cheap compared to psychological
treatments. E; However, some patients may benefit from
the fact of just talking to a doctor during consultations as
it could help.
- SSRIs; block the re-uptake of serotonin at
the presynaptic membrane, increasing
serotonin concentration at receptor sites
on the post synaptic membrane. E.g Proza
to increase levels of neurotransmitter
serotonin to regulate mood and anxiety
Media attachments
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Mind Maps for free with GoConqr? Learn more.