5132773
Biological Etiology of Major Depressive Disorder
- Biochemdical
- Neurotransmitter
- serotonin
hypothesis
- Lacasse and Leo
(2005)
- lack of evidence that any depressed
person has low levels of serotonin
- no baseline balanced level of
serotonin to measure against
- Cannot compare the level of serotonin
before and after having depression
- Cannot compare the level of serotonin
before and after having depression
- no baseline balanced level of
serotonin to measure against
- common analogy for what is wrong with using the e ectiveness
of a treatment as support for a causal explanation
- headaches are successfully treated by aspirin, but we do not have any
theory suggesting that headaches are caused by a lack of aspirin
- headaches are successfully treated by aspirin, but we do not have any
theory suggesting that headaches are caused by a lack of aspirin
- lack of evidence that any depressed
person has low levels of serotonin
- Sarek, 2006
- tianeptine, a drug commonly used in Europe
and South America to treat depression
- opposite action to fluoxetine
- prevention of neuronal damage due to stress
- prevention of neuronal damage due to stress
- opposite action to fluoxetine
- tianeptine, a drug commonly used in Europe
and South America to treat depression
- significant in the pharmaceutical industry
- medical treatment
- medical treatment
- Lacasse and Leo
(2005)
- serotonin
hypothesis
- Hormone
- cortisol
- reactivity to stress
- Burke et al., 2005
- meta- analysis of studies connecting
cortisol with depression
- difference in reactivity to stress between
depressed and non-depressed people
- non- depressed people
- cortisol levels rise and fall rapidly
- cortisol levels rise and fall rapidly
- depressed people
- more blunt reaction and remain
under stress for longer
- more blunt reaction and remain
under stress for longer
- non- depressed people
- meta- analysis of studies connecting
cortisol with depression
- Hormone--> reactivity to stress--> depression
- Depression--> change in hormone--> more reactive to stress
- Burke et al., 2005
- history of many negative life events
- Cutuli et al., 2010
- homeless children
- age: 4-7
- significant correlation between
high levels of cortisol and a
history of many negative life
events
- Negative life event--> Hormone~> Depression
- homeless children
- Cutuli et al., 2010
- reactivity to stress
- Correlation does not indicate causation
- Change in hormone --> depression
- Depression --> change in hormone
- Change in hormone --> depression
- Provide medical treatment
- easy to measure
- synthetic
- can be directly injected into bloodstream
- easy to measure
- cortisol
- Neurotransmitter
- Genetics
- Evolution
- Hagen et al. (2004)
- signal need
- elicit help from others in the social group
- signal need
- Logical
- e.g. the point that most suicides by depressed individuals are preceded by the threat of suicide, which therefore signals a need for help and attention
- e.g. the point that most suicides by depressed individuals are preceded by the threat of suicide, which therefore signals a need for help and attention
- impossible to test experimentally
- genetic basis of this evolved behaviour
- Hagen et al. (2004)
- Genes
- Twin
Study
- Kendler et al., 2006
- Swedish
- over 42 000 participants
- Large Sample
Size
- Large Sample
Size
- telephone interviews
- Self-reporting
bias
- Participants may not have the
insight to symptoms
- Self-reporting
bias
- diagnose depression on the basis of (a) the presence of most of the DSM-IV symptoms or (b) having had a prescription for antidepressants
- concordance rates among monozygotic twins of 44% for female and 31% for male, compared with 16% and 11% for female and male dizygotic twins respectively
- indicate a strong genetic
component
- Not purely genetic (if
yes,monozygotic concordance
rates would be much higher)
- Not purely genetic (if
yes,monozygotic concordance
rates would be much higher)
- Swedish
- Kendler et al., 2006
- Gene
Mapping
- Caps et al. (2003)
- Relationship between 5-HTT gene and
depression after stressful events
- Both genes and environmental
factors are under investigation
- Difficult to conclude the gene is a
major contribution to depression
- Unclear how environmental
factors influence genes
- Difficult to conclude the gene is a
major contribution to depression
- Compared participants with normal 5-HTT genes
and a mutation with shorter alleles
- Large proportion of population
carries the mutation of 5-HTT gene
- 43%
- Participant with shorter alleles: more likely
to become depressed after stressful event
- Vulnerability to depression after stress events
- Vulnerability to depression after stress events
- Large proportion of population
carries the mutation of 5-HTT gene
- Both genes and environmental
factors are under investigation
- 847 Caucasian New Zealanders
- large sample size
- large sample size
- Self-report on depression
- Cross checking with friends
- Cross checking with friends
- Relationship between 5-HTT gene and
depression after stressful events
- Caps et al. (2003)
- Ethics
- Having the genes does not
equal having the disorder
- Having the genes does not
equal having the disorder
- Confusing
- Levinson (2005)
- short allele on 5-HTT acts in a similar way of drugs
improve the symptoms of depression (e.g. Prozac); it
hinders reuptake of serotonin
- short allele on 5-HTT acts in a similar way of drugs
improve the symptoms of depression (e.g. Prozac); it
hinders reuptake of serotonin
- Levinson (2005)
- Predict who is vulnerable to depression
- Provide special treatment to
prevent having the disorder
- Provide special treatment to
prevent having the disorder
- Levinson
(2005)
- the gene is more likely to make individuals
more sensitive to stressful life events
- the gene is more likely to make individuals
more sensitive to stressful life events
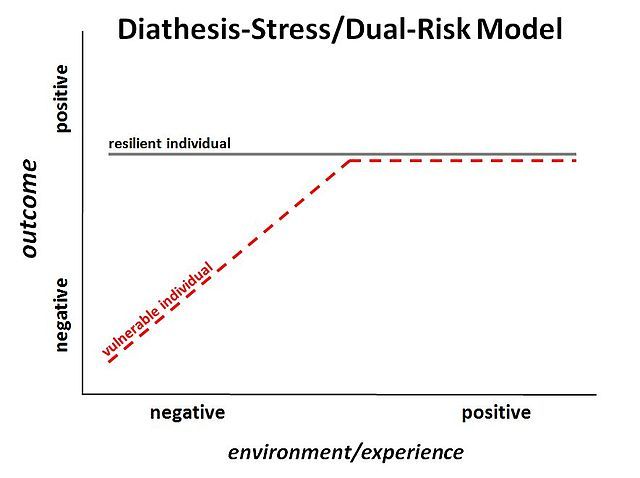
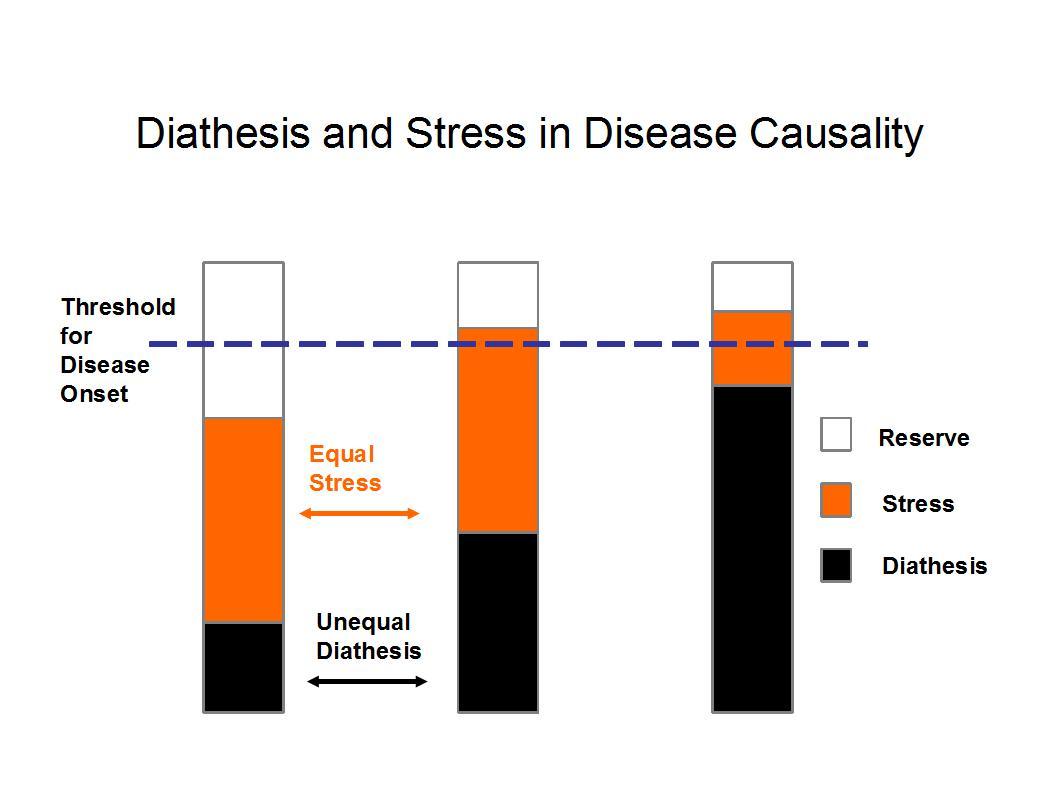
- Diathesis–stress model
- explain behavior as a predispositional vulnerability
together with stress from life experiences
- Lazarus (1993)
- if the combination of the predisposition and the stress exceeds a threshold,
the person will develop a disorder
- if the combination of the predisposition and the stress exceeds a threshold,
the person will develop a disorder
- Lazarus (1993)
- explain behavior as a predispositional vulnerability
together with stress from life experiences
- Twin
Study
- Evolution
Media attachments
{kind=link}
{kind=link}
Want to create your own Mind Maps for free with GoConqr? Learn more.