
8216360
Description

| Question | Answer |
| AP Axial Toes Evaluation Criteria | ANATOMY: distal phalynx -> half of metatarsals CRITERIA: IP and MTP joints open no overlap from adjacent digits equal concavity on either side of digits POSITIONING: CR 10 caudal @ 3rd MTP joint |
| AP Axial Toe Evaluation Criteria | ANATOMY: distal phalanges -> half the metatarsal CRITERIA: open MTP and IP joints equal concavity on either side of phalange no soft tissue or bone superimposition from unaffected toes POSITIONING: CR 10 caudal @ affected PIP joint |
| What's wrong with this AP Axial Toe? | DIP is closed - toe is flexed essential anatomy is coned off |
| more concave to the medial side of the 1st digit - foot/toe is rotated laterally | |
| more concave to the lateral side of the 1st digit - foot/toe is rotated medially | |
| more concavity on the medial side of 1st digit - foot/toe rotated laterally | |
| AP Oblique Toes Evaluation Criteria | ANATOMY: distal phalanges -> half of metatarsals CRITERIA: twice as much soft tissue to one side of digits vs. other more cancavity of digits to one side side of digit closest to IR should be almost straight POSITIONING: CR perpendicular @ MTP joint |
| What's wrong with this oblique toe? | toe appears more lateral than oblique excessive obliquity |
| Errors? | toe appears more AP than oblique insufficient obliquity |
| Lateral Toe Evaluation Criteria | ANATOMY: distal phalanges -> half of metatarsal CRITERIA: condyles of the proximal phalanx are superimposed side of digit closest to IR is mostly straight majority of soft tissue/concavity on the side farthest from IR POSITIONING: CR perpendicular @ PIP of interest |
| What's wrong with this lateral toe? | the unaffected digits were not drawn away from the affected digit too much superimposition |
| Errors? | unaffected toes need to be drawn away from affected toe not true lateral - toes appear more oblique insufficient lateral rotation |
| AP Axial Foot Evaluation Criteria | ANATOMY: distal phalanges -> 1/3 of talus superimposing the calcaneus CRITERIA: equal space and concavity between digits TMT and navicular-cuneiform joint spaces appear open POSITIONING: CR 10 caudal @ 3rd MTP joint |
| What's wrong with this AP Axial Foot? | TMT joint spaces are closed the CR was not aligned parallel with these joint spaces |
| Errors? | cuneiform joint spaces appear closed insufficient CR angle |
| AP Oblique Foot Criteria | ANATOMY: distal phalanges -> calcaneus -> distal malleoli of ankle CRITERIA: minimal overlapping of adjacent phalanges and metatarsals Sinus tarsi and 5th MT tuberosity are well visualized POSITIONING: CR perpendicular @ 3rd MTP joint |
| excessive obliquity phalanges and metatarsals are very superimposed | |
| insufficient obliquity lateral cuneiforms and cuboid have closed joint spaces | |
| Lateral Foot Criteria | ANATOMY phalanges, MT's, tarsals, calcaneus, 1'' of distal lower leg CRITERIA MT heads are superimposed Tibiotalar joint is open distal fibula superimposed by half of distal tibia proximal talar domes are aligned long axis of foot is 90 degrees to the long axis of lower leg POSITIONING |
| proximal tibia is elevated talar domes aren't superimposed superiorly to inferiorly | |
| toes elevated, heel down lateral talar dome is more anterior than the medial talar dome | |
| heel elevated, toes down lateral talar dome is more anterior vs. the medial talar dome | |
| AP Ankle Criteria | ANATOMY distal 4th of tibia and fibula and talus CRITERIA medial mortise joint appears open Tibiotalar space is open Tibia superimposed 1/2 of distal fibula POSITIONING CR perpendicular @ midway between malleoli |
| External rotation | |
| internal rotation | |
| proximal lower leg is elevated *Tibiotalar joint is closed | |
| Mortise Ankle Criteria | ANATOMY lateral and medial malleoli in profile CRITERIA mortise joint is open tibia superimposes 1/4 distal fibula Tibiotalar joint is open POSITIONING CR perpendicular @ midway between malleoli foot dorsiflexed, and internally rotated 15-20 degrees |
| insufficient obliquity | |
| excessive obliquity | |
| 45 Degree Oblique Ankle Criteria | ANATOMY distal 1/4 fibula and tibia and talus CRITERIA fibula is free of superimposition Tibiotalar joint is open sinus tarsi is open POSITIONING CR perpendicular @ midway between malleoli foot dorsiflexed, internally obliqued 45 degrees |
| Errors? oblique | insufficient obliquity |
| Errors? | distal leg elevated insufficient obliquity |
| Errors? | distal leg elevated |
| Errors? | excessive medial obliquity |
| Lateral Ankle Mediolateral Evaluation Criteria | ANATOMY talus, 1'' of 5th MT tuberosity, and distal 1/4 of tibia and fibula CRITERIA Tibiotalar joint appears open distal fibula is superimposed by the posterior half of the distal tibia proximal aspects of talar domes are superimposed POSITIONING CR perpendicular @ medial malleolus |
| heel elevated toes down the fibular head is more posterior talar domes are not superimposed anteriorly to posteriorly | |
| knee elevated talar domes aren't superimposed superiorly to inferiorly fibular head is more anterior | |
| toes elevated heel down distal fibula is tucked under the talar domes and appears more anterior | |
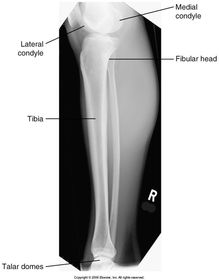
| AP Lower Leg evaluation criteria | ANATOMY entire tibia/fibula, both ankle joint and knee joint CRITERIA tibia superimposes 1/4 of fibular head and 1/2 of distal fibula knee and Tibiotalar joints are closed* POSITIONING CR perpendicular to mid-leg |
| Errors? | leg is laterally rotated |
| Errors? | anatomy is cut off - centered too high leg is internally rotated |
| Lateral lower leg evaluation criteria | ANATOMY tibia, fibula, knee, and ankle CRITERIA tibia superimposes 1/2 fibular head fibular midshaft is free of superimposition of the tibia knee and Tibiotalar joints are closed* POSITIONING CR perpendicular to midleg |
| Errors? | leg is externally rotated fibular head is not superimposed by tibia |
| Errors? | leg is internally rotated fibula is almost completely superimposed by the tibia |
| AP Knee evaluation criteria | ANATOMY entire knee joint, femoral epicondyles in profile, tibia superimposes 1/2 of fibular head, 1/4 of proximal lower leg is seen CRITERIA patella lies just proximal to the femoral patellar surface ICF is only partially seen POSITIONING CR 3-5 cephalic for hypersthenic CR perpendicular for sthenic CR 3-5 caudal for asthenic all @ 1/2'' distal to apex of patella |
| Errors? | Excessive internal rotation fibular head is seen with minimal superimposition by the proximal tibia patella is shifted medially medial condyle appears larger |
| Errors | CR is angled too cephalic the fibular head is elongated |
| Error? | knee is overflexed intercondylar fossa is demonstrated, so we know the knee is flexed to some degree |
| Errors? | CR is angled too caudal fibular head is elongated and is projected more superiorly into the tibial condyle ***if the fibular head has moved up, the CR angle was caudal*** |
| Errors? | leg is externally rotated patella is shifted away from midline fibular head is superimposed by tibial condyle medial condyle appears larger |
| Errors? | excessive caudal CR angle *fibular head |
| Internal Oblique Knee evaluation criteria | ANATOMY entire knee joint demonstrated, fibular head in profile CRITERIA open knee joint fibular head is 0.5'' distal to tibial plateau lateral femoral condyle is in profile POSITIONING CR centering is same as AP knee is in 45 degree internal oblique |
| Errors? | excessive obliquity knee appears almost lateral femoral head is completely free of superimposition |
| Errors? | CR is excessively angled knee joint space is narrowed tibial plateau is not level |
| External Oblique Knee evaluation criteria | ANATOMY entire knee joint, 1/4 of proximal lower leg CRITERIA fibular head is aligned with anterior edge of tibia medial femoral condyle in profile POSITIONING CR same as AP knee is in 45 degree external oblique |
| errors? | insufficient obliquity fibula is not completely superimposed by the anterior edge of tibia |
| errors? | excessive external obliquity knee appears almost lateral |
| Lateral Knee evaluation criteria | ANATOMY entire knee joint CRITERIA femoral condyles superimposed patella in profile femoropatellar joint open tibia superimposed 1/2 of fibular head POSITIONING CR 5-7 cephalic @ 1'' distal to medial epicondyle |
| errors? | over rotation - posterior femoral condyles aren't superimposed, fibular head is almost free of superimposition, patella is superimposed partially no cephalic angle - distal femoral condyles are not superimposed |
| errors? | distal lower leg and foot are elevated *the medial femoral condyle follows the medial condyle of the tibia, when the foot is elevated the medial condyle/tibial condyle are seen distal to the lateral condyles *fibular head has moved superiorly* |
| errors? | excessive cephalic angle *femoral head and lateral femoral condyle are elongated and projected inferiorly *medial femoral condyle and tibial condyle are projected superiorly joint space is closed |
| errors? | proximal femur is elevated *knee is underrotated *medial femoral condyle and tibial condyle are projected posteriorly and superiorly *lateral femoral condyle and femoral head are projected inferiorly and anteriorly |
| errors? | knee is over flexed femoropatellar joint is closed |
| errors? | under rotation *adductor tubercle *fibular head |
| PA or AP Views for Intercondylar Fossa evaluation criteria | ANATOMY ICF shown in profile CRITERIA knee joint is open patella outline is superimposed by distal femur tibia superimposes 1/2 of fibular head POSITIONING CR parallel to tibial plateau |
| errors? | knee is overflexed *patella isn't superimposed by distal femur, the apex is seen within the ICF *fibular head is elevated |
| errors? | knee is externally rotated *any time the knee is rotated when we're looking for the ICF, the ICF will appear narrow as if it's being closed* |
| errors? | CR angled too caudal *any time there's too much caudal angle, the fibular head will migrate superiorly* knee is over flexed *patellar apex is seen within the ICF* |
| error? | CR angled too cephalic *extreme cephalic angle will cause the fibular head to migrate inferiorly, and the ICF will start to close* |
| AP Proximal Femur and Hip evaluation criteria | ANATOMY femoral head, acetabulum, proximal 1/3 of femur CRITERIA greater trochanter, femoral head/neck in profile lesser trochanter not visible/minimally visible ischial spine is aligned with pelvic brim POSITIONING CR perpendicular to midfemoral neck rotate foot internally 15 degrees |
| error? | lesser trochanter is in profile foot is externally rotated |
| error? | leg is externally rotated - lesser trochanter patient is rotated towards the affected hip - left iliac wing is wide and the obturator foramen is narrowed sacrum and coccyx aren't lined up with MSP |
| error? | leg externally rotated patient rotated away from affected hip - sacrum and coccyx aren't vertical with symphysis pubis |
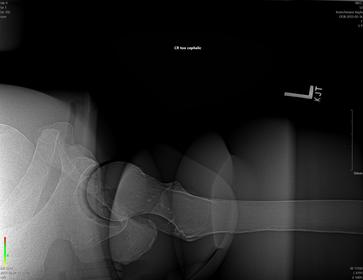
| Frog leg Lateral Proximal Femur and Hip evaluation criteria | ANATOMY proximal 1/3 of femur, femoral head, neck, acetabulum, and part of pelvis CRITERIA lesser trochanter in profile medially femoral neck demonstrated on end greater trochanter is at the same level as the femoral head femoral shaft is not distorted POSITIONING CR perpendicular to mid femoral neck OR aligned with IR for lateral femur |
| error? | excessive lateral rotation *greater trochanter is seen medially* |
| error? | Excessive flexion of the knee will place the greater trochanter medial and proximal, and will foreshorten the femoral neck patient is rotated towards affected hip femoral head/neck are elongated sacrum/coccyx aren't lined up with symphysis right iliac wing is wider, left obturator foramen is open |
| error? | not enough flexion of knee will cause the frogleg hip to appear more like an AP with the greater trochanter placed laterally |
| X-Table Lateral Hip and Proximal Femur | same evaluation criteria |
| error? | CR was not angled cephalic enough *caudal angle will place the femoral heads closer together* |
| error? | CR was angled too cephalic femoral head/neck are projected within the pelvis |
| AP Axial SI Joints evaluation criteria | ANATOMY open SI joints CRITERIA sacrum is elongated and SI joints are not foreshortened POSITIONING CR 30-35 cephalic @ 2'' inferior to ASIS |
| error? | excessive cephalic angle sacrum is elongated |
| error? | insufficient cephalic angle *superior half of SI joints are closed, inferior half are open* |
| Posterior Oblique SI Joints evaluation criteria | ANATOMY open SI joint of interest is seen on the upside CRITERIA ilium and sacrum aren't superimposed POSITIONING CR perpendicular @ 1'' medial to upside ASIS |
| errors? | excessive obliquity is marked by the narrow ilium of pelvis, SI joint is projected through the ilium, and the midline of sacrum has shifted away from MSP |
| errors? | insufficient obliquity ilium is superimposed by the sacrum SI joint is closed minimally |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
0 comments
Want to create your own Flashcards for free with GoConqr? Learn more.