17978824
8. Remodelling
Description
No tags specified
Slide Set by Chloe Cavarretta, updated more than 1 year ago
More
Less
|
|
Created by Chloe Cavarretta
almost 7 years ago
|
|
Resource summary
Slide 1
Learning Outcomes: L16-17
Explain the organisation of the extracellular matrix (ECM) and the different ECM components involved
Explain the mechanisms governing ECM assembly
Describe how cell function can be regulated by the ECM
Explain the transcriptional control of embryonic stem cells and the defining characteristics of stem cells
Describe how stem cells can be induced to generate specific differentiated cell types and how differentiated function can be experimentally tested
Explain how pluripotency can be induced in somatic cells (SCNT and iPS cells)
Give examples of the therapeutic potential of stem cells
Slide 2
The ECM
Tissues composed of cells and often ECM
ECM composed of proteins and proteoglycans
Connective tissues form framework of vertebrate body but amounts vary for different organisms
Physical properties of different tissues can vary from hard structures (bone) to transparent (cornea)
Cells have physical interaction with ECM: integrins on cell membrane
Interaction important for cell survival
Slide 3
ECM: Support Structure
Inert scaffold to stabilise physical structure of tissues
Helps define cellular phenotype of cells residing within it: what cell is and what it does
Acts as storage compartment for cell signalling factors
Slide 4
Composition of ECM: Collagens
~25% of total mamamalian proteins- most abundant protein
Homo- or hetero- trimers-> form triple helical structure (alpha chains)
Give tissues tensile strength
Gly-X-Y repeats for aa seq (X and Y often proline, hydroxyproline, hydroxylysine and glycine essential every 3rd residue)
Vitamin C essential cofactor- hence hydroxylation important for collagen function
Effects of impaired collagen synthesis through vitamin C deficiency
Lack of collagen/inappropriately synthesised= lose structural support, prone to easy wounding and don’t repair well
Slide 5
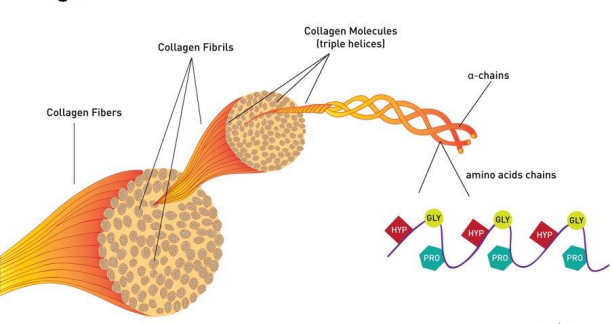
Structure of Collagen Fibres
{kind=link}
Slide 6
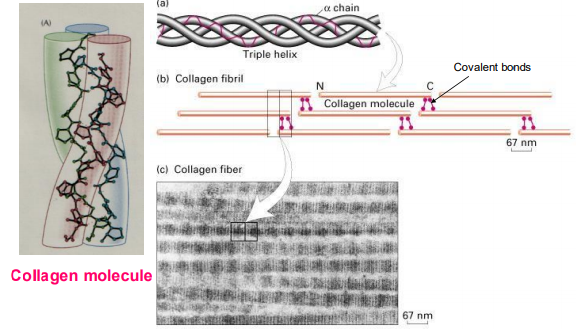
Collagens: Why is Glycine Needed?
Small aa that enables triple helical twisting to form a collagen molecule
Collagen molecules associate with each other through covalent bonding to form fibril
Fibrils associate with eachother to form fibers
{kind=link}
Slide 7
Different Types of Collagen
Collagens are diverse but there are some similarites in their structure
Different organisations of homo or hetero trimers but always 3 alpha chains
Different functions depending on structure and location in body
Slide 8
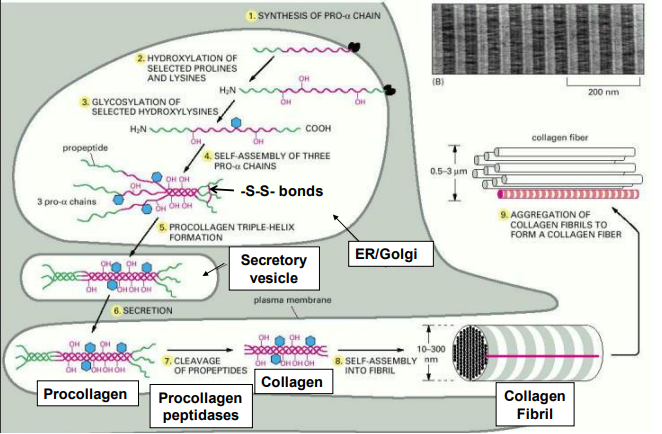
Collagen Synthesis + Secretion from Cell
Synthesis through ribosomes into pro-alpha chain
Hydroxylation of predominantly lysine and proline- uses vitamin C
Glycosylation of alpha chain
Spontaneous self assembly of alpha chain into triple helix (pro-peptide at end that dont form helix)
Procollagen secreted into extraceullular space
Cleavage of pro-peptides forms collagen which forms fibrils then fibres outside cell
Slide 9
{kind=link}
Collagen Synthesis + Secretion from Cell
Slide 10
Collagen Gene Mutations
Osteogenesis Imperfecta (OI, brittle bone disease)
Caused by mutations in α1(I) or α2(I) genes
Dermatosparaxis- inherited disorder
Causes fragile and loose skin with substantial bruising and bleeding
Caused by mutations in N-terminal propeptidase that removes pro-peptides in type I and III collagen
Proteolytic processing of procollagen required for collagen assembly into fibrils
N-terminal propetidase= Metalloproteinase ADAMTS-2
Slide 11
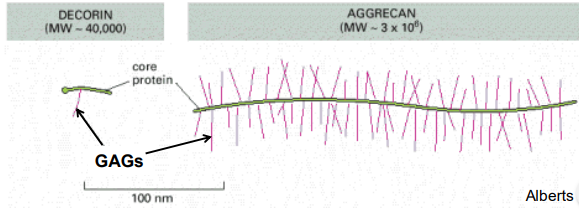
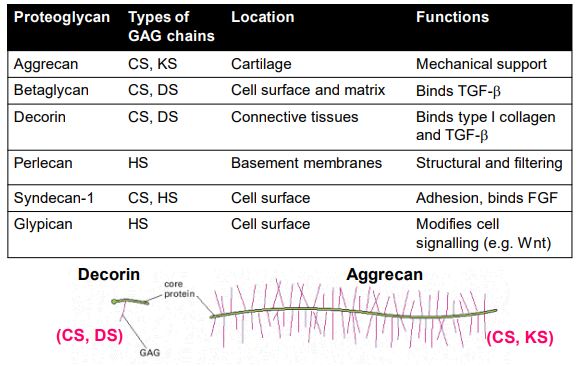
ECM Components: Proteoglycans + GAGs
Glycosaminoglycans (GAGs) attached to core protein to form proteoglycan (except hyaluronan)
Eg. Aggrecan= core protein decorin with lots of GAGs attached
Large space filling molecule, hydrated water trapping structure
Space filling function and compressive strength important in cartillage
Aggrecan lost in arthiritis
Slide 12
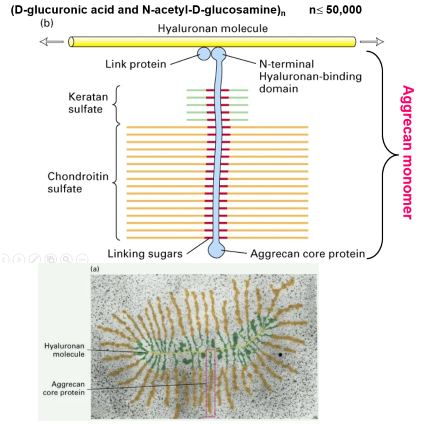
Aggrecan Structure
{kind=link}
Slide 13
Four Classes of GAGs
GAGs formed by polymerisation of specific dissacharides and modifications:
1. Hyaluronan (HA)- binds other proteoglycans to build bigger structures
2. Chondroitin Sulphate (CS)
3. Heparan Sulphate (HS)
4. Keratan Sulphate (KS)
Slide 14
ECM Components: Proteoglycans + GAGs
Variety of different proteoglycans enabled by different combinations of core proteins with GAGs and numbers of GAGs affect their function
Some basic structures->
{kind=link}
Slide 15
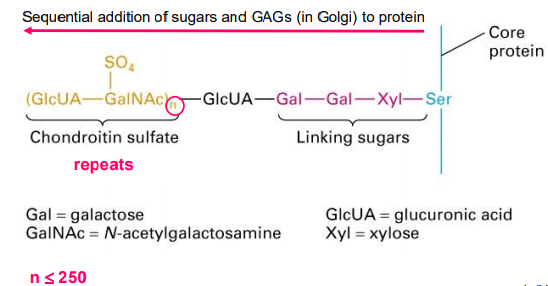
Assembly of Proteoglycans
{kind=link}
Linking sugars enable attachment of GAGs to core protein
n= multiples of GAGs away from core protein
Slide 16
Hyaluronan: GAG that Links Proteoglycans
Hyaluronan made of repeating disaccharide units ~5000
Hyaluronan binds proteoglycan (aggrecan) through link proteins
Multiple proteoglycans can bind to hyaluronan
{kind=link}
Slide 17
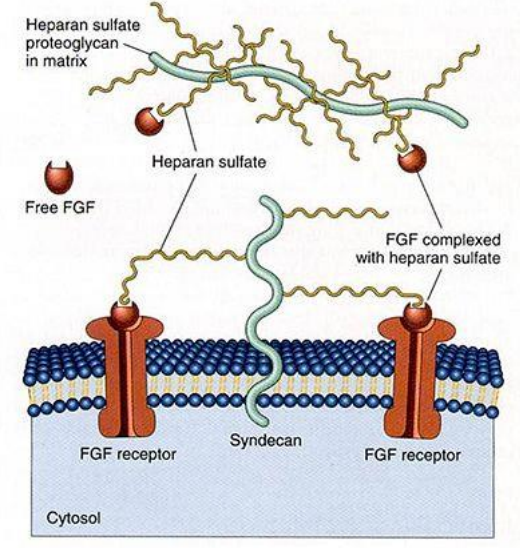
Proteoglycans and Cell Signalling
Major role in signalling between cells- they bind various secreted molecules, enhance or inhibit signalling activity of growth factors
FGF signalling (fibroblast):
Heparan sulphate proteoglycan (HSPGs) help control FGF signalling strength- FGF binding FGF-R regulated by its presentation to receptor by proteoglycan
Free FGF doesnt have bioactivity
Enhance signal= FGF binds HS proteoglycan (syndecan) in cell membrane- depending on proteoglycan expression levels and proximity to FGF-R can present FGF to receptor and increase the signal
Inhibit signal= HSPGs free in extracellular space may not be near receptors and can sequester FGF
Slide 18
Proteoglycans and FGF Signalling
{kind=link}
Slide 19
ECM Components: Elastin
{kind=link}
Gives elasticity to tissues, help regulate tissue function
Consists of covalently linked monomers
Elasticity to connective tissues:
Elastin is the dominant ECM component in arteries ~50%
Also in lungs and elastic ligaments
Maintains structure and shape
Slide 20
{kind=link}
Elastin Associated Disorders
Cutis Laxa
Rare inherited disorder of connective tissues
Skin inelastic and hangs loosely
Caused by mutation in genes that affect elastin formation and function
May cause hypermobility of joints
Slide 21
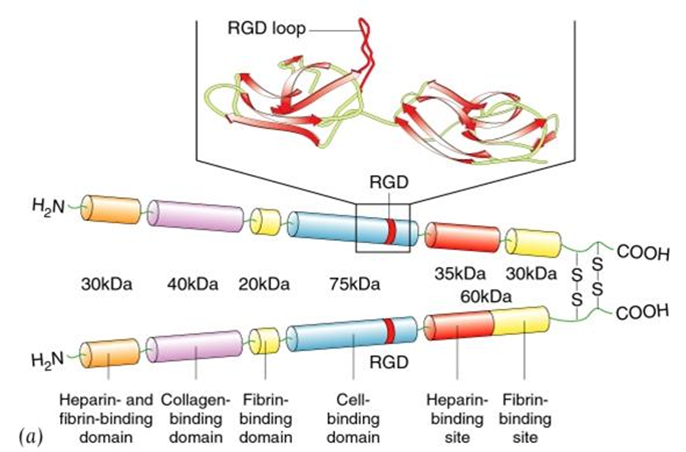
ECM Components: Fibronectin
{kind=link}
Large glycoprotein, helps matrix organisation
Multi-adhesive protein (binds many things)
Homodimer has many binding motifs for proteoglycans, cells, collagen
RGD domain= recognised by integrins- enables interactions between cells
Slide 22
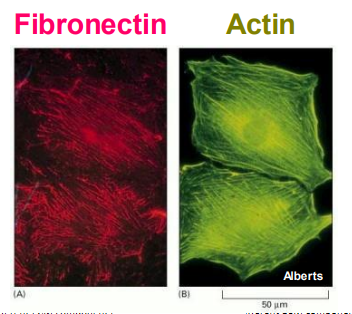
Regulation of Cell Behaviour by ECM
{kind=link}
Cells need to attach to ECM to grow and proliferate (and survive)- blood cells dont
=Anchorage Dependence
Mediated by integrins and signals they generate
Intracellular actin cytoskelton overlaps with extracellular fibronectin via integrin interactions
Slide 23
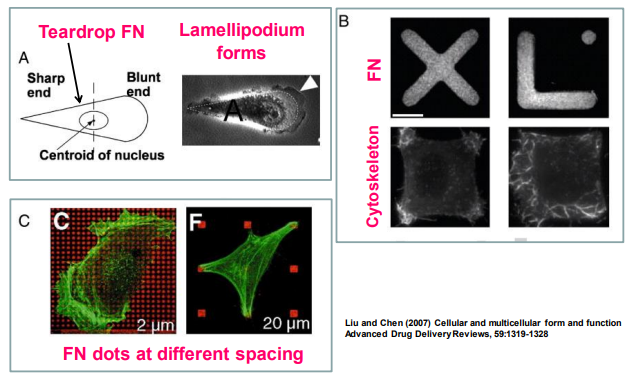
Regulation of Cell Behaviour by ECM
How ECM geometry and organisation can regulate cell function
Experiment: Cells grown on different fibronectin shapes
Make fibronectin cell sized and shape into tear drop, apply one cell (only thing that can bind)
Cell takes up teardrop shape- orders actin cytoskeleton into that shape and forms lamellipodium
Pulled into shape of migrating cell- so wants to migrate, ECM controls function
{kind=link}
Slide 24
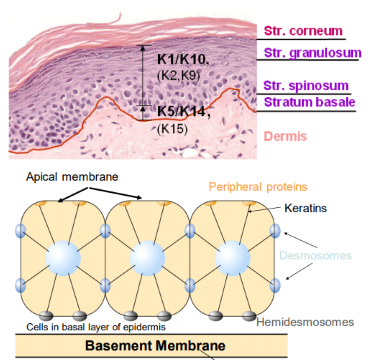
The Basal Lamina: Basement Membrane
Basement membrane is a specialised ECM structure made up of different ECM components
Separates epidermis (epidermal cells) from dermis (skin)
Dermis made from collagen network underlying the connective tissue
{kind=link}
Slide 25
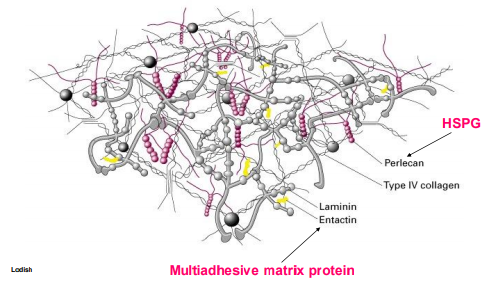
The Basal Lamina: Basement Membrane
Basement membrane composed of:
Entactin- multiadhesive protein
Perlecan- HSPG
Lamin
Type IV collagen- forms sheet like structure
Acts as selective barrier for cell movement
{kind=link}
Slide 26
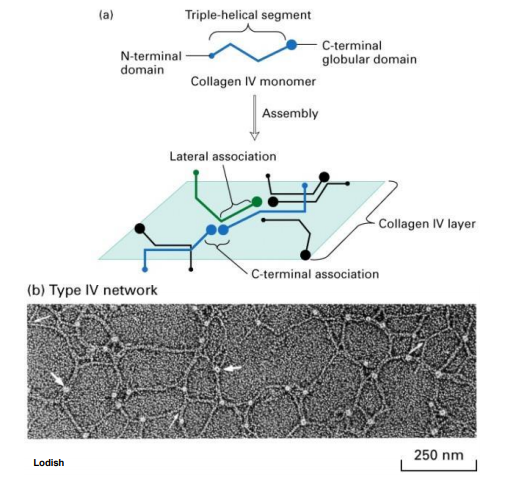
Basement Membrane Components
Type IV collagen:
Defines back bone of flat sheet like structure due to its organisation
Triple helical structure of alpha chains
Monomer has globular head (C-), kinked structure
Head allows end-on-end associations and lateral associations= forms planar network of collagen
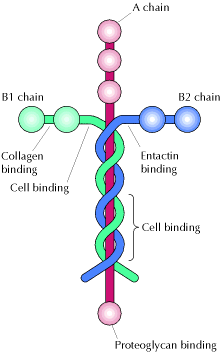
Laminin:
Crucifix shaped protein
Binds to many other things: HSPG, collagen, fibronectin, entactin
Slide 27
Basement Membrane Components
{kind=link}
{kind=link}
Slide 28
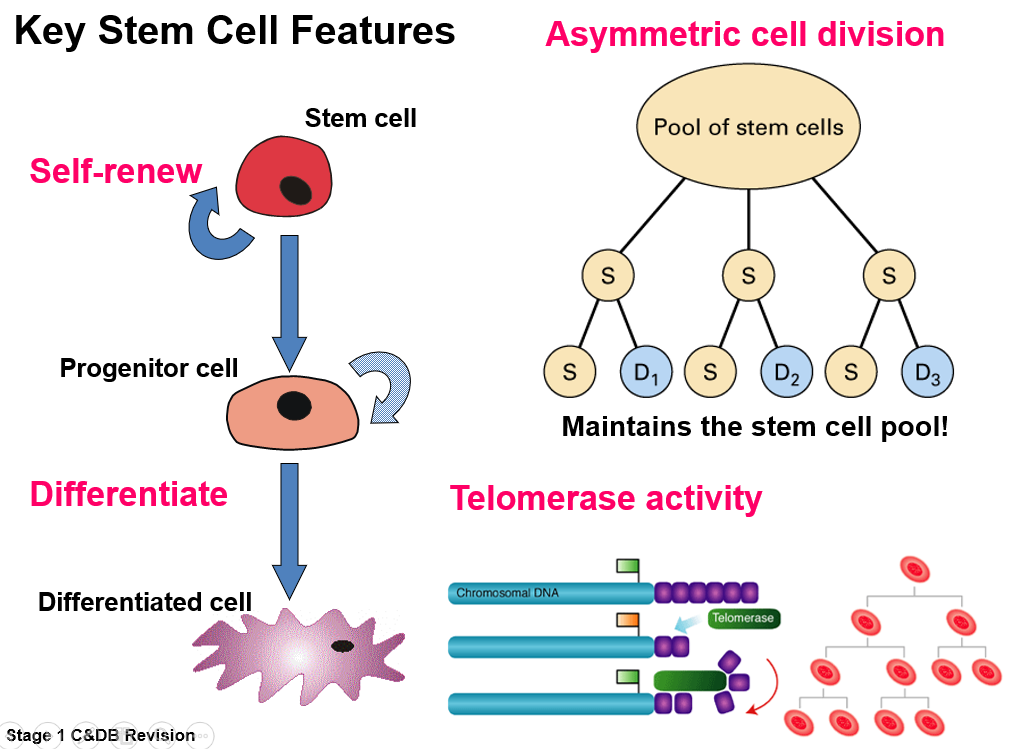
Stem Cell Key Features
Self renewal- Divide asymmetrically to give rise to another stem cell (maintain stem cell pool) and transit amplifying cell (differentiate)
Differentiation- goes through precursor stage and becomes specialised cell
ESC have ability to live longer- increased telomerase activity, more rounds of cell division
Slide 29
Stem Cell Key Features
{kind=link}
Slide 30
Potency of ESC
Potency= repertoire of different cell types SCs can differentiate into
Totipotent= Ability to develop into entire organism
Including supportive cells (extraembryonic tissues), enable embryo to implant and survive(umbilical cord and placenta)
Stages(early embryogenesis): fertilised egg, daughter cells upto day 4 following fertilisation, before blastocyst
Pluripotent=Ability to develop into virtually every cell type (3 germ layers)
Don't form supportive tissue needed for foetal development, unable to generate new organism on their own
Stages: ES cells of inner cell mass in blastocyst
Slide 31
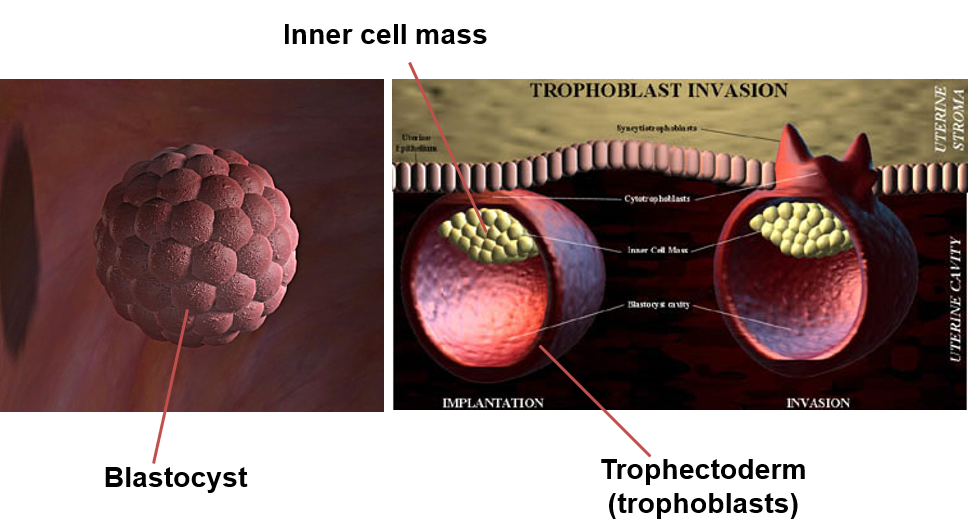
Blastocyst Structure
Fluid filled ball of cells
Outer layer= trophectoderm from Exe tissue (trophoblasts)
Inner cell mass= where pluripotent ESCs reside
{kind=link}
Slide 32
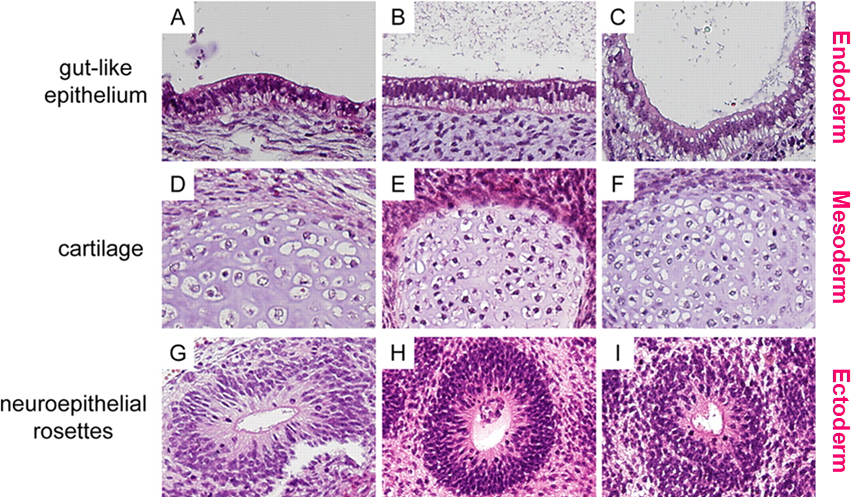
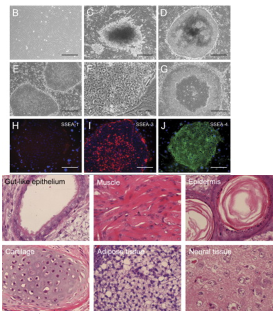
Determining Pluripotency-Teratoma Assay
In vivo method of determining pluripotency , teratoma=benign cancer with tissues from all 3 germ layers
Experiment:
Take population of suggested pluripotent SCs,inject into immunocompromised mouse
If pluripotent-> develops teratoma, all 3 germ layers
Analysis:
Histological analysis- look at sections of teratoma, do we see structures/cells from each germ layer eg gut-like epithelium, cartilage, neuroepithelial rosettes
Stem cell assay- Histological analysis alone not enough, need to create a defect and see if suggested pluripotent cells restore functionality in defect
Slide 33
Histological Analysis
{kind=link}
Slide 34
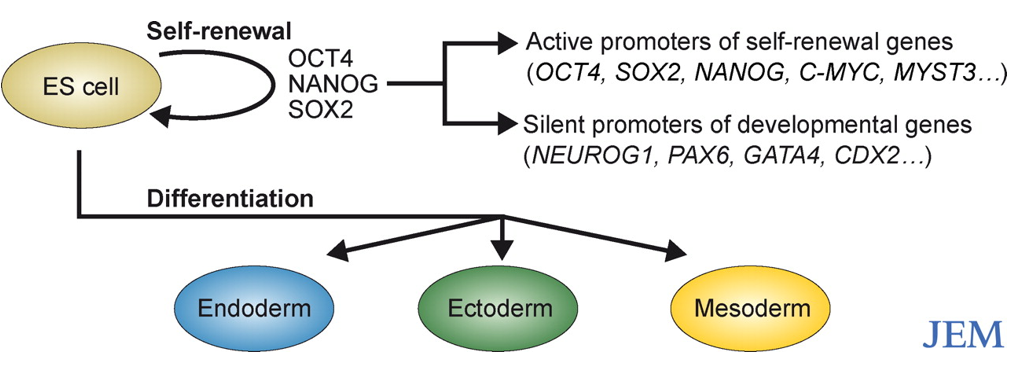
Transcriptional Control of ESCs
Pluripotent TFs: Oct4, Nanog, Sox2 (act collectively to regulate pluripotency)
Expressed early in pluripotent ESCs in inner cell mass
How they regulate:
Activate pluripotency associated pathways, active promoters of self-renewal genes
Suppress pathways that progress cell differentiation, silent promoters of developmental genes
Upon differentiation ESCs lose expression of TFs
Slide 35
Transcriptional Control of ESCs
{kind=link}
Slide 36
Therapeutic Potential of ESCs
Generate specific cell types/tissue structures-replace worn/diseased body parts:
Neurodegenerative diseases
Diabetes
Corneal defects
Cardiovascular diseases
Musculoskeletal disorders
Other applications include:
Toxicity testing- replace animal testing?
Model systems- 3D co-culture system engineered from stem cells that can differentiate and mimic developmental processes
Potential difficulties:
Need differentiation of cells into specific cell types to form functional tissues
Need ALL cells to COMPLETELY differentiate- no pluripotent SC which could give rise to a teratoma
Slide 37
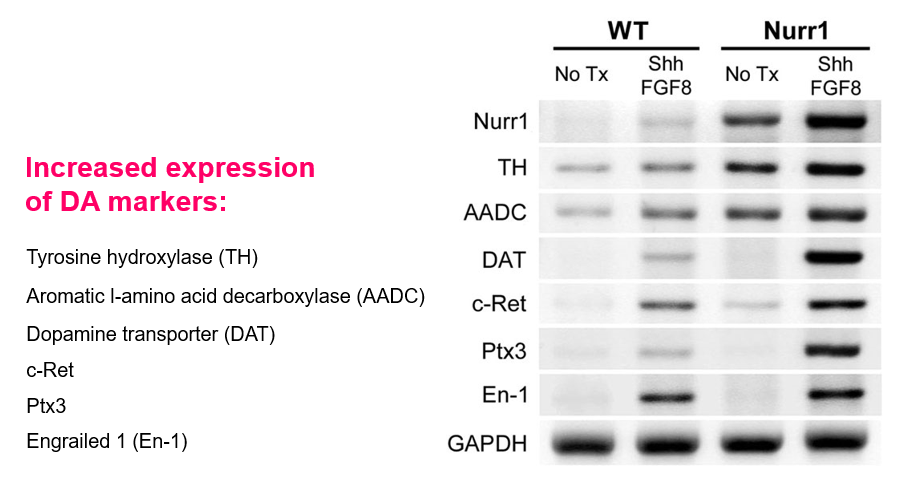
Therapeutic Potential: Parkinson's
Characteristic of Parkinson's= Dopamine producing neurones in CNS die off
Loss of dopamine binding causes neurones to fire out of control
TF Nurr1 involved in differentiation of neuronal precursors into dopamine-producing neurones
Growth factors FGF8 and sonic hedgehog (Shh) are required for dopamine producing neurones in normal midbrain
TFs and GFs= signals that can be applied to stem cells and induce differentiation
Slide 38
Therapeutic Potential: Parkinson's
Experiment: Indication of formation of dopamine producing neurones from ESCs
GAPDH= loading control
WT ESC lines exposed to GFs- increased expression of markers for DA-producing neurones
ESC lines that overexpress Nurr1 (TF) exposed to GFs- significant further increase of expression of markers
{kind=link}
Slide 39
Indicated ESCs may be forming DA-producing neurones, need functional test to be sure
Experiment(functional test):
Use animal model where DA-producing neurones killed off to mimic Parkinson's
Inject stem cells (from previous) and look for restored functionality- removal of Parkinson's characteristic
Therapeutic Potential: Parkinson's
Slide 40
Therapeutic Potential
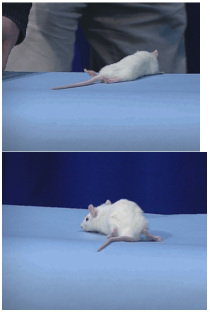{kind=link}
Example of transplantation of neuronal cells differentiated from human ESCs
Paralysis in rat model- equivalent to spinal cord injury
Following transplantation, injection of neurones into spinal cord lesions and restore some function
Slide 41
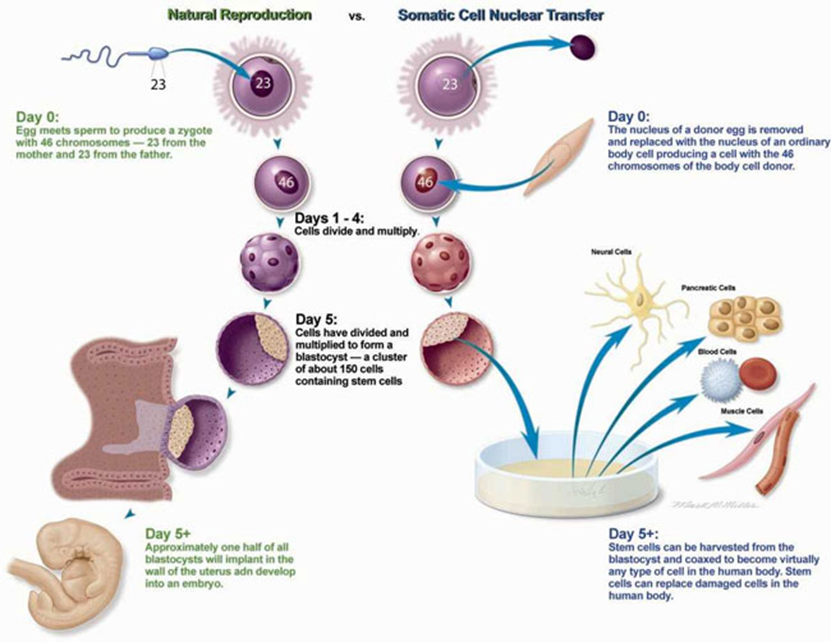
Therapeutic Cloning and ESCs
Somatic cell nuclear transfer(SCNT):
Fusion of a somatic (adult) cell nucleus with emptied egg(enucleated)
Reverts adult cell back to its pluripotent state
Technique used to create dolly the sheep, used to create an organism = reproductive cloning
When used to generate a blastocyst from which ICM pluripotent cells are isolated and expanded in vitro= therapeutic cloning
Differentiate them for therapeutic processes, genetically identical to donor nucleus so wont be rejected
Slide 42
Natural Reproduction vs SCNT
{kind=link}
Slide 43
Adult Stem Cells
Effectively in every tissue and maintain tissue ability to self-renew
Ability deteriorates with age
Tissue repair and remodelling
Multipotent
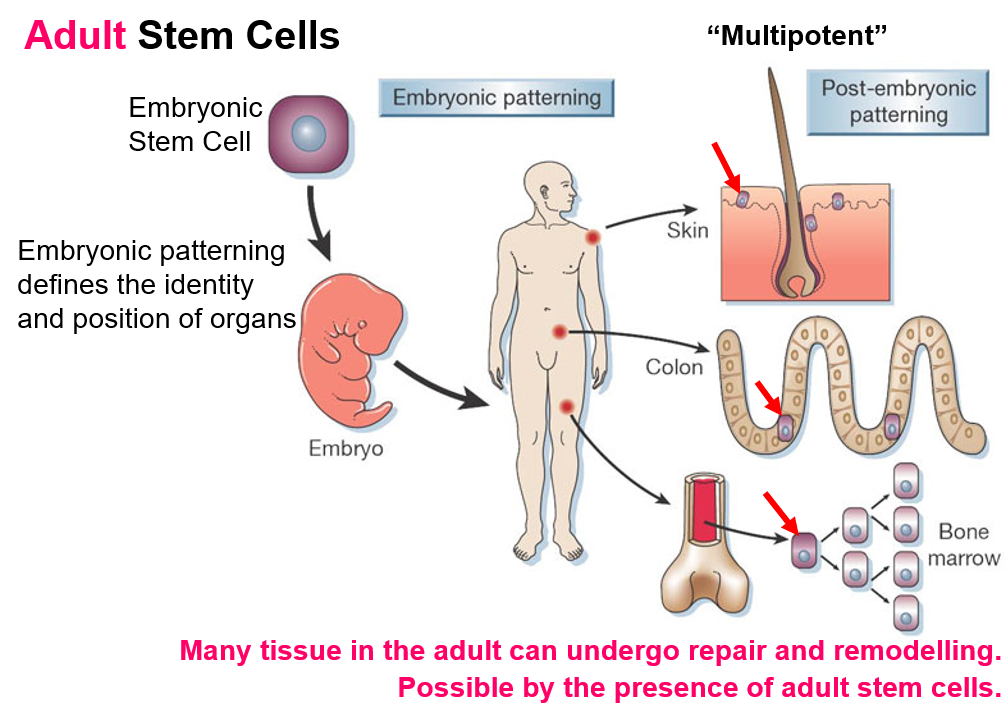{kind=link}
Slide 44
Adult Stem Cell: Multipotent
Stem cells that can differentiate into more than one cell type
But more restricted differentiation potential than pluripotent stem cells
Generally have ability to differentiate into the cells of tissues in which they reside
Therapeutic potential:
Allows use of autologous cells
Fewer safety concern than ESCs- no risk of teratoma
Fewer ethical concerns than ESC- no creating embryos in clinic
Examples of adult stem cell for therapeutic processes:
Haematopoietic stem cells (HSC)
Mesenchymal
Epidermal- skin grafts/burns
Neural- Spinal cord injury
Limbal (corneal)- treat corneas
Slide 45
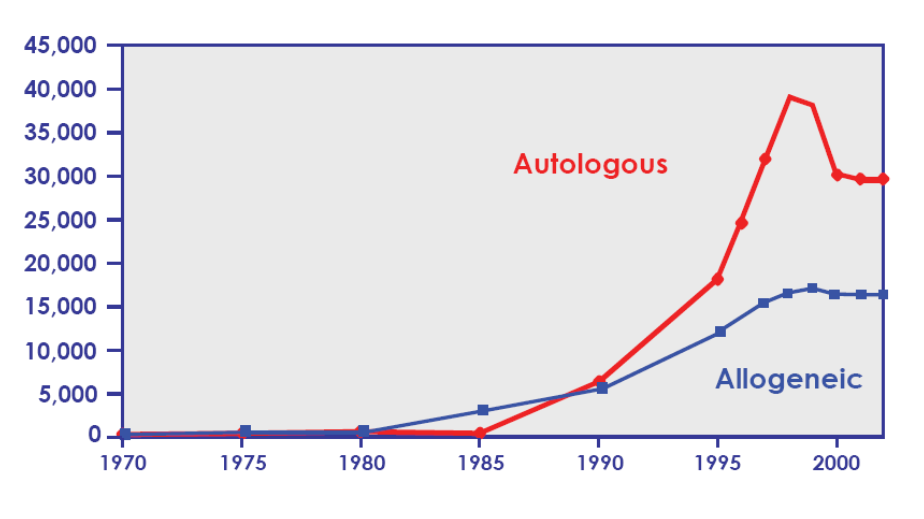
Haematopoietic Stem Cells: HSCs
HSC transplants are effectively blood and marrow transplants
Massive increase in autologous (own cells) and allogenic (different donor to recipient) blood marrow transplants through the years
More autologous in recent years
{kind=link}
Slide 46
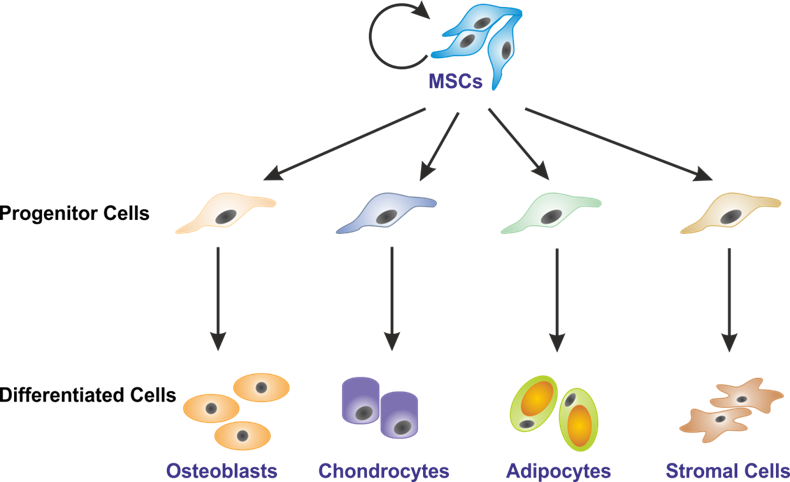
Mesenchymal Stem Cells (MSC)
{kind=link}
Found in BM and give rise to structural tissues like bone and cartilage
Good for diseases that affect skeleton-arthiritis
Osteogenesis Imperfecta (OI, brittle bone disease):
Genetic, mutation in genes coding type I collagen
Potential treatment using adult SC therapy
Allogenic BM transplant using MSC
Restore strength of skeleton to some extent and enables normal collagen production
Slide 47
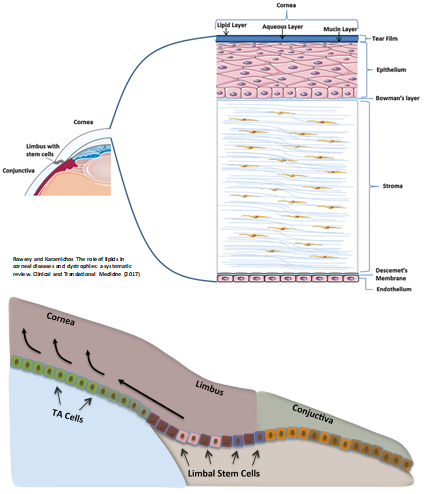
Cornea and Limbal Stem Cells
Cornea made up of collagen (stroma) surrounded by epithelium tissue (outer layer of cornea)
Limbus region stem cells give rise to epithelial corneal cells that maintain health and support corneal structure
{kind=link}
Slide 48
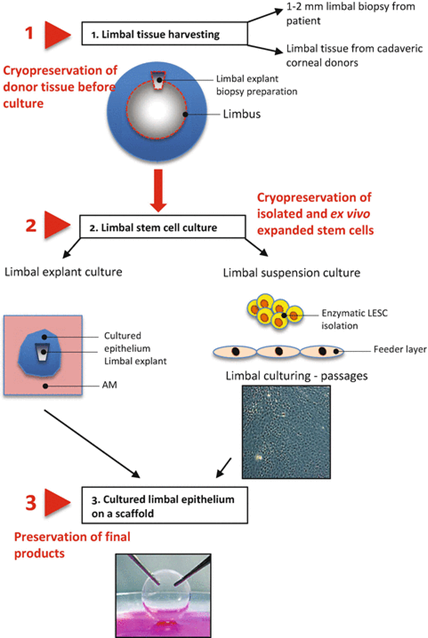
Limbal Stem Cell Therapy
Corneas subject to damage/injury- loss of corneal function/damage may benefit from limbal stem cell therapy to restore lost function
How it works:
Cornea and surrounding limbus- biopsy to get viable limbal stem cells
Expand cells by growing in petri dish
Replacing 3D structure:
Use amniotic membrane- has same physical properties as cornea (translucent, type I collagen)
Populate membrane with limbal stem cells + induce differentiation
Can transplant whole cornea structure
Slide 49
Limbal Stem Cell Therapy
{kind=link}
Slide 50
Limbal Stem Cell Therapy
2 different approaches:
Generate enough limbal stem cells to use in cell based therapy- injection of stem cells into damaged cornea
Generate stem cells to create 3D structure that replaces cornea
Histological analysis= look for markers of epithelial corneal cells
Applications of limbal stem cell therapy:
Limbal stem cell deficiency- cell based therapy
Loss of corneal structure- injury/burns- 3D transplant
Corneal clouding due to aging- transplant
Slide 51
Induced Pluripotent Stem Cells (iPS)
Oct-4, Sox2 and Nanog TFs and others involved in regulating ESC pluripotency, understanding regulatory control of pluripotency underpinned iPS cell development:
Introducing genes associated with ESC plutipotency (TFs) into somatic cells eg fibroblasts could reprogram somatic cell to pluripotent stem cell
Introduction of 4 or fewer factors was sufficient
Some genes include: Oct-4, Sox-2, Nanog, Lin28, Klf4, c-Myc
Slide 52
Induced Pluripotent Stem Cells (iPS)
Experiment: Using viral delivery system, introduced factors into somatic fibroblasts
Look for formation of stem-cell like colonies (compact clusters)
Do induced pluripotent stem cells express telomerase, ESC surface markers, and differentiate into 3 germ layers (Teratoma)?
{kind=link}
Slide 53
Induced Pluripotent Stem Cells (iPS)
Issues:
Reprogramming typically inefficient (<1%)- depends on number of cells that take up virus/vector carrying reprogramming factors and number of ones that do that actually undergo reprogramming
Use viral delivery systems- safety concern
Use oncogenes (cMyc)- cancer risk
Epigeneitc memory of parent cell (unlike SCNT)- can return back to ESC but retain epigenetics of original fibroblast
Teratoma risk
Slide 54
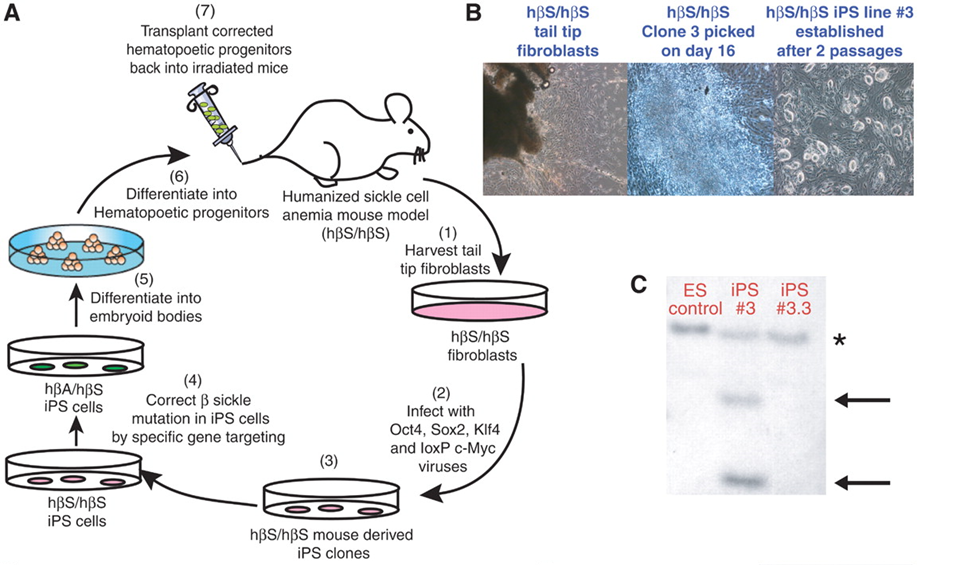
Example of iPS Use
Treat sickle cell anaemia in mouse model: Caused by mutation in haemoglobin gene
How it works:
Isolate cells from mouse with anaemia and expand them
Infect cells with reprogramming factors and reverse back to pluripotent state
Correct mutation using genetic engineering (CRISPR/Cas9) and differentiate into haemoglobin carrying cells
Put back in mouse model and look for restored functionality
Slide 55
Example of iPS Use
{kind=link}
Slide 56
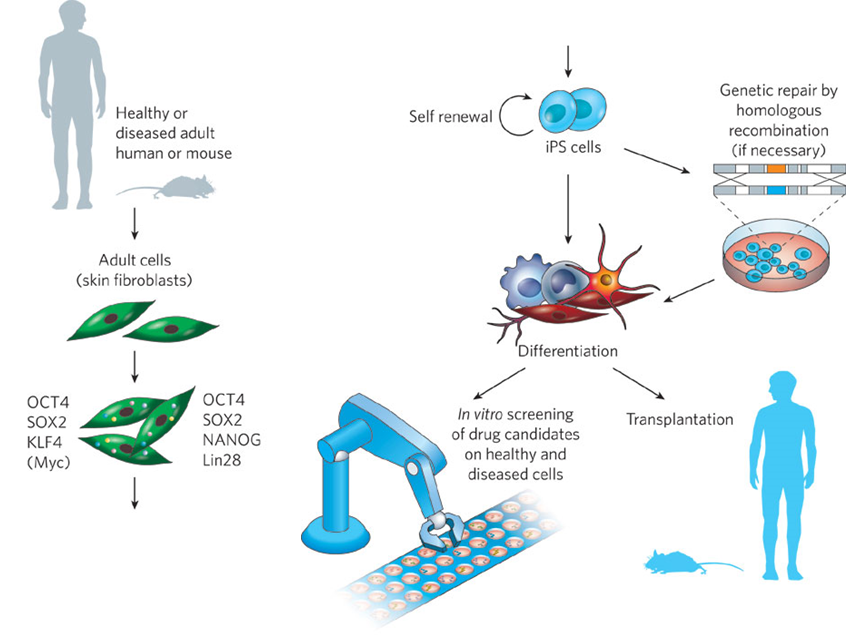
Potential of iPS Cells
Take own cells, revert back to ESC and differentiate (with or without genetic mutation)
Grow differentiated cell type and replace back into individual
No risk of immunological rejection- same genetics
Used for transplant or in vitro screening
{kind=link}
Want to create your own Slides for free with GoConqr? Learn more.