20546060
Description
Flashcards by Raziel Rosas, updated more than 1 year ago
|
|
Created by Raziel Rosas
over 4 years ago
|
|
| Question | Answer |
| Risk factors for pneumonia | 1. Impaired lung defense: poor cough / gag reflex (illness or drug induced), impaired mucociliary transport (smoking, cystic fibrosis), immunisuppression (steroids, chemotherapy, hiv, DM) 2. Increased risk of aspiration |
| Most common etiology in pneumonia | No organism identified in 75% of hospitalized cases, and 90% of ambulatory cases |
| Common organism in community acquired pneumonia | 1. Typical: S. Pneumoniae, M. Catarrhalis, H. Influenzae, S.aureus, group A streptococcus. 2. Atypical: M. Pneumoniae, chlamydophilia pneumoniae, Legionella pneumophilia 3. Viral: influenza, adenovirus |
| Common organism in nosocomial pneumonia | Enteric gram negative bacilli (E.coli), pseudomonas, S.aureus |
| Common organism in pneumonia by aspiration | Oral anaerobes (bacteroides), enteric gran negative bacili (E. Coli), S. Aureus, gastric contents (chemical pneumonitis) |
| Common organism in immunocompromised patients pneumonia | Pneumocystis jiroveci, fungi (cryptococcus), nocardia, CMV, HSV, TB |
| Common organism in alcoholic patients with pneumonia | Klebsiella, enteric GNB, S. Aureus, Oral anaerobes aspiration), TB |
| Treatment for clinically suspected HAP with no increase in likehood of MRSA and not at high risk of mortality | B-lactam/ B-lactamase inhibitor / antipsudomonal cephalosporin / antipseudomonal carbapenem /antipseudomonal fluoroquinolne |
| Treatment for clinically suspected HAP with increase likehood of MRSA and not at high risk of mortality | B-lactam/ B-lactamase inhibitor / antipsudomonal cephalosporin / antipseudomonal carbapenem /antipseudomonal fluoroquinolne/ monobactam plus MRSA coverage |
| Treatment for clinically suspected HAP with high risk of mortality or recipient of Iv antibiotics in last 90 days | Two of the following (avoid 2 b-lactams): B-lactam/ B-lactamase inhibitor / antipsudomonal cephalosporin / antipseudomonal carbapenem /antipseudomonal fluoroquinolne/ monobactam / amino glycosides + plus MRSA coverage |
| Clinically suspected VAP in units where empiric MRSA coverage and double antipseudomonal/ gram negative coverage are appropriate | One of: B-lactam/ B-lactamase inhibitor / antipsudomonal cephalosporin / antipseudomonal carbapenem /lmonobactam +plus one of : antipseudomonal fluoroquinolone / aminoglycoside or polymyxins +plus MRSA coverage |
| Glasgow coma scale | Eye response: 4 spontaneous, 3 open eyes to voice, 2 open eyes to pain, 1 no eye opening Verbal response: 5 oriented, 4 confused, 3 inappropriate words, 2 incomprehensible sounds, 1 no response Motor response: 6 obeys commands, 5 localized to pain, 4 withdraws from pain, 3 flexion to pain, 2 extension to pain, 1 no response |
| Indications for intubation in trauma | 1.- Depressed LOC ( the patient cannot protect airway) GCS <8 2.- need for hyperventilation 3.- severe maxillofacial trauma 4.- need for pharmacologic paralysis for evaluation or management |
| Signs of airway obstruction | *agitation , confusion, universal choking sign, * respiratory distress, * failure to speak, dysphonia, stridor * cyanosis |
| Medications that can be delivered via ETT | NAVEL: *N: naloxone * A: atropine *V: ventolin (salbutamol) *E: epinephrine *L: lidocaine |
| 4 P, indications of intubation | Patency , protection of the airway, positive pressure ventilation need, predicted deterioration |
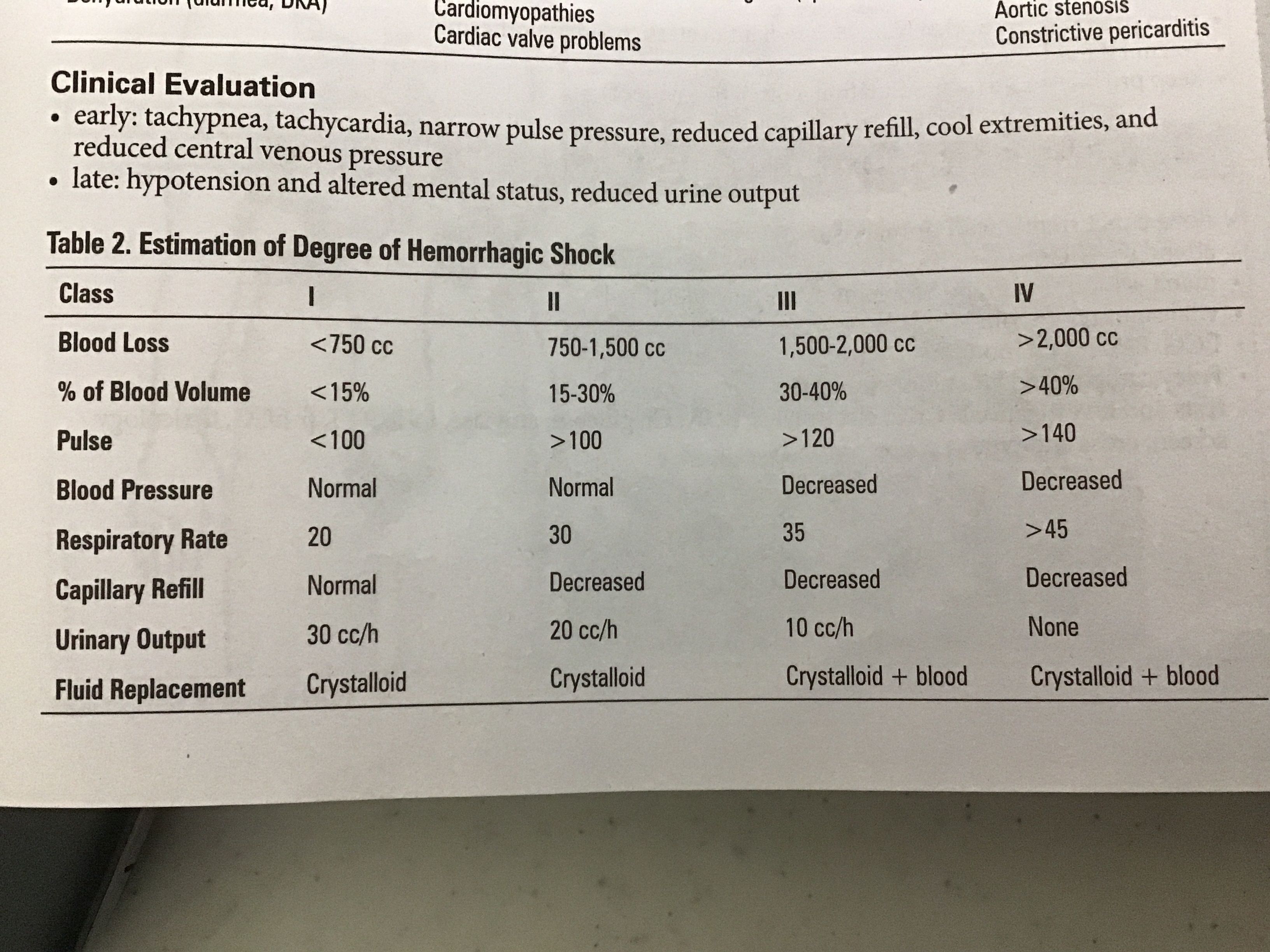
| Early and late signs of shock in the clinical evaluation of circulation | Early: tachypnea, tachycardia, narrow pulse pressure, reduced capillary refill, cold extremities, reduced central venous pressure Late: hypotension, altered mental status, reduction of the urinary outcome |
| Estimation of degree of hemorrhagic shock |
Image:
Image (binary/octet-stream)
|
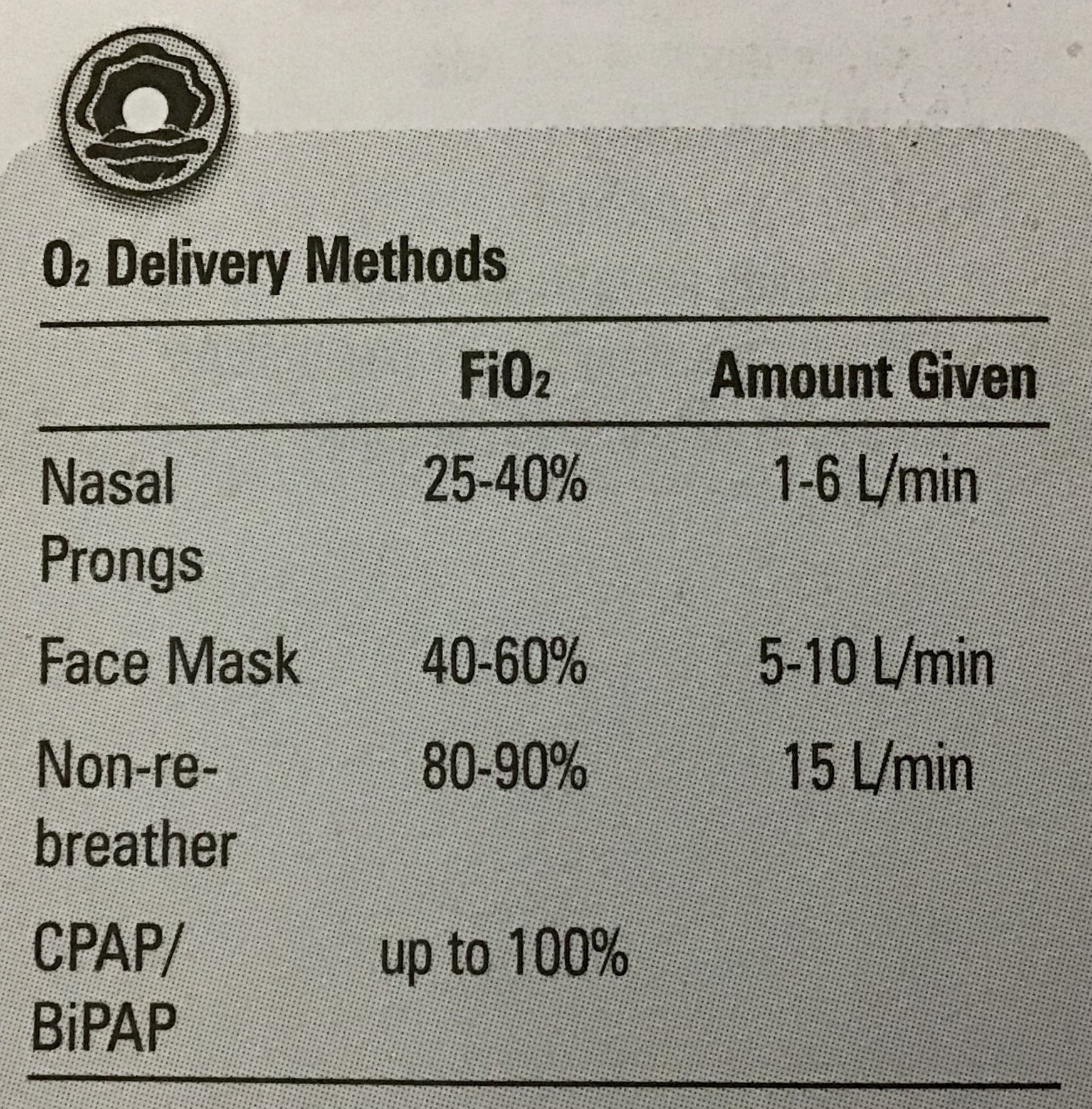
| O2 deliver methods | |
| Contraindications to foley insertion | Blood at urethral meatus, scrotal hematoma, high riding prostate at DRE |
| Best imaging modality for intracranial injury | Non contrasted CT head |
| Signs of increased ICP | * deterioration LOC ( hallmark) * deteriorating respiratory patter * Cushing reflex ( hypertension, hyperventilation or irregular and low heart rate) * lateralizing CNS signs * seizures * papilledema ( is a late sing) * N/V and headache |
| Confusion assessment method (CAM) for diagnosis of delirium | Need: 1+2+( 3 or 4) 1.- acute onset and fluctuating course 2.- inattention 3.- disorganized thinking 4.- altered level of consciousness : hyperactive or hypoactive |
| Dyspepsia : definition, common etiology, history and physical exams, investigations and management | D:Predominant epigastric pain lasting at least one month. E:#1functional (idiopathic), PUG, GERD, gastritis. H: Age, associated symptoms ( red flags) and drugs (NSAID) PE: adenophaty, abdominal mass/ organomegaly, carnetts sign(means muscular pain) I: CBC, liver enzymes, calcium, H.pylori, %US M: for GERD and PUG, H2 inhibitors and PPI inhibitors. For functional disease use pro kinetic |
| Dyspepsia red flags | (Raise suspicion of gastric malignancy), weight loss, Persistent vomiting, progressive dysphagia, odynophagia, hematemesis (also anemia or iron deficiency unexplained, jaundice, abdominal mass or adenophaty, family history of GI cancer, previous gastric surgery |
| Dx of gestational DM | Step1: perform a random non fasting 50g OGCT: 1 hr PG < 7.8 normal 1hr PG > 11.1 GDM Step 2: if 7.8- 11.1 perform fasting 75g OGTT : FPG >5.3 1hr PG > 10.6 2hr PG > 9.0 Test all the pregnancy around 24-28wk |
| Management aims in GDM | In preconception: commence folic acid 3 months prior and evaluate retinopathy, neuropathy and CAD FPG <5.3mmol/L (95mg/dL) 1hr PG <7.8 mmol/L (140mg/dL) 2hr PG <6.7 (120) this is the most efficient to determinate pregnancy outcomes In labor 3.9 to 7mmol/L Postpartum BGq6hrs if 8mmol/L restart insulin 2/3 dose |
| Complications in GDM | Maternal complications: HTN, preeclampsia, polyhidramnios, hypoglycemia, CKA, diabetic coma, pyelonephritis, UTI. Fetal complications: macrosomia, IU growth restriction, fetal lung immaturity, preterm labor, stillbirth, birth trauma, hypoglycemia, hyperbilirrubinemia, hypocalcemia, polycythemia. |
| Complications in DM in pregnancy ( but not in GDM) | Spontaneous abortion, ventricular and septal defects, NTD, cystic kidney, anal atresia and sacral agenesia |
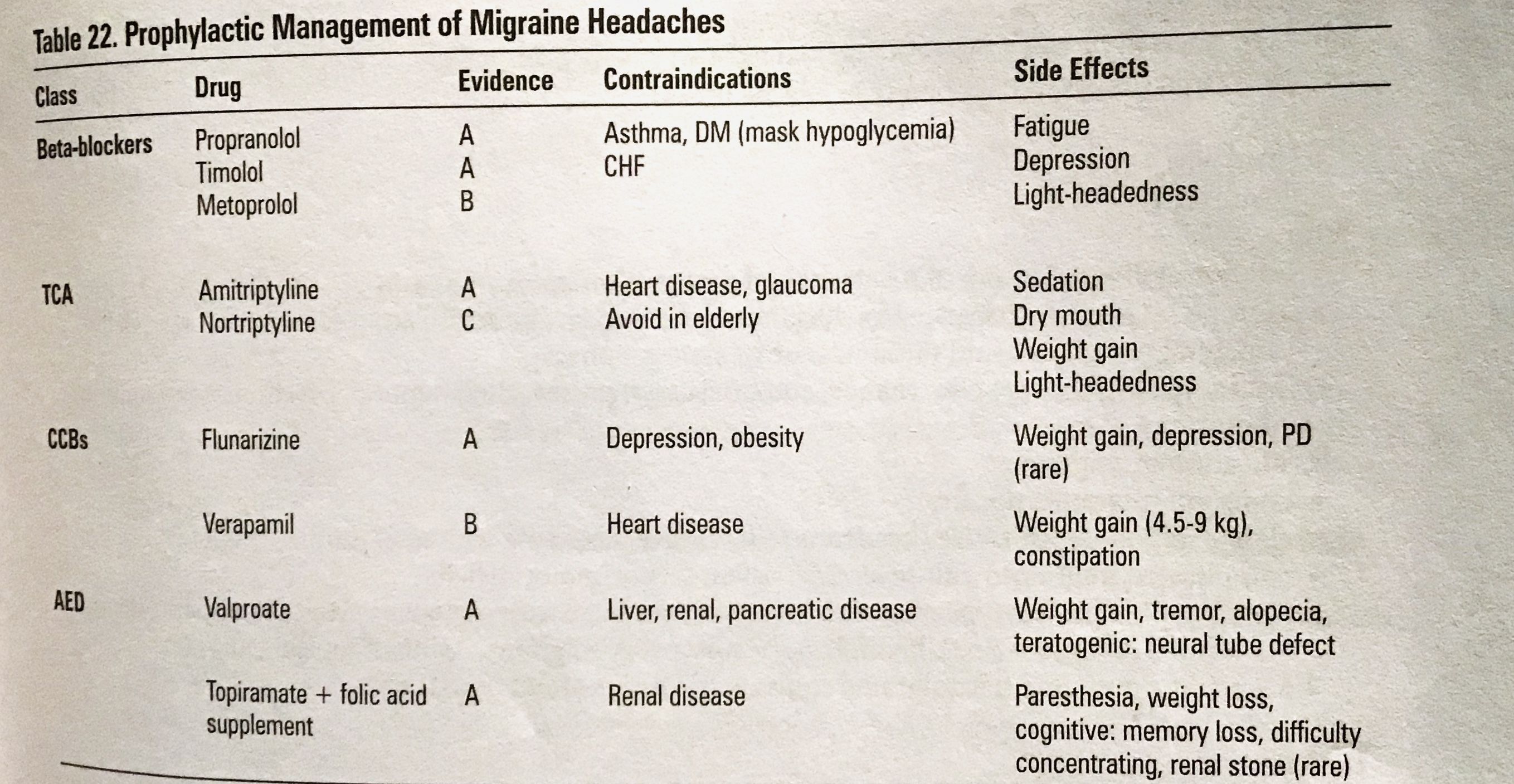
| Prophylactic management of migraine headache | |
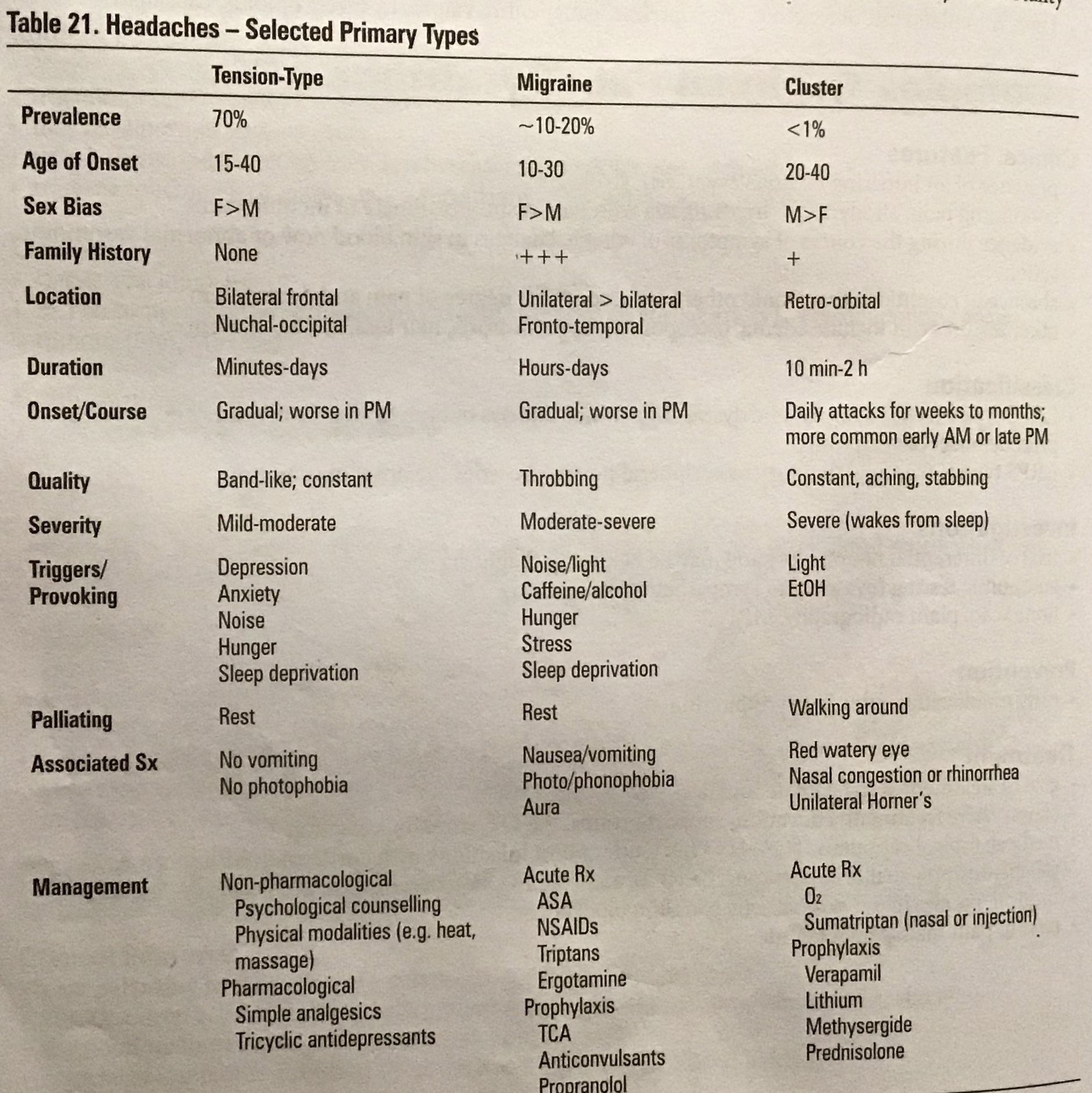
| Headache primary types (differences) | |
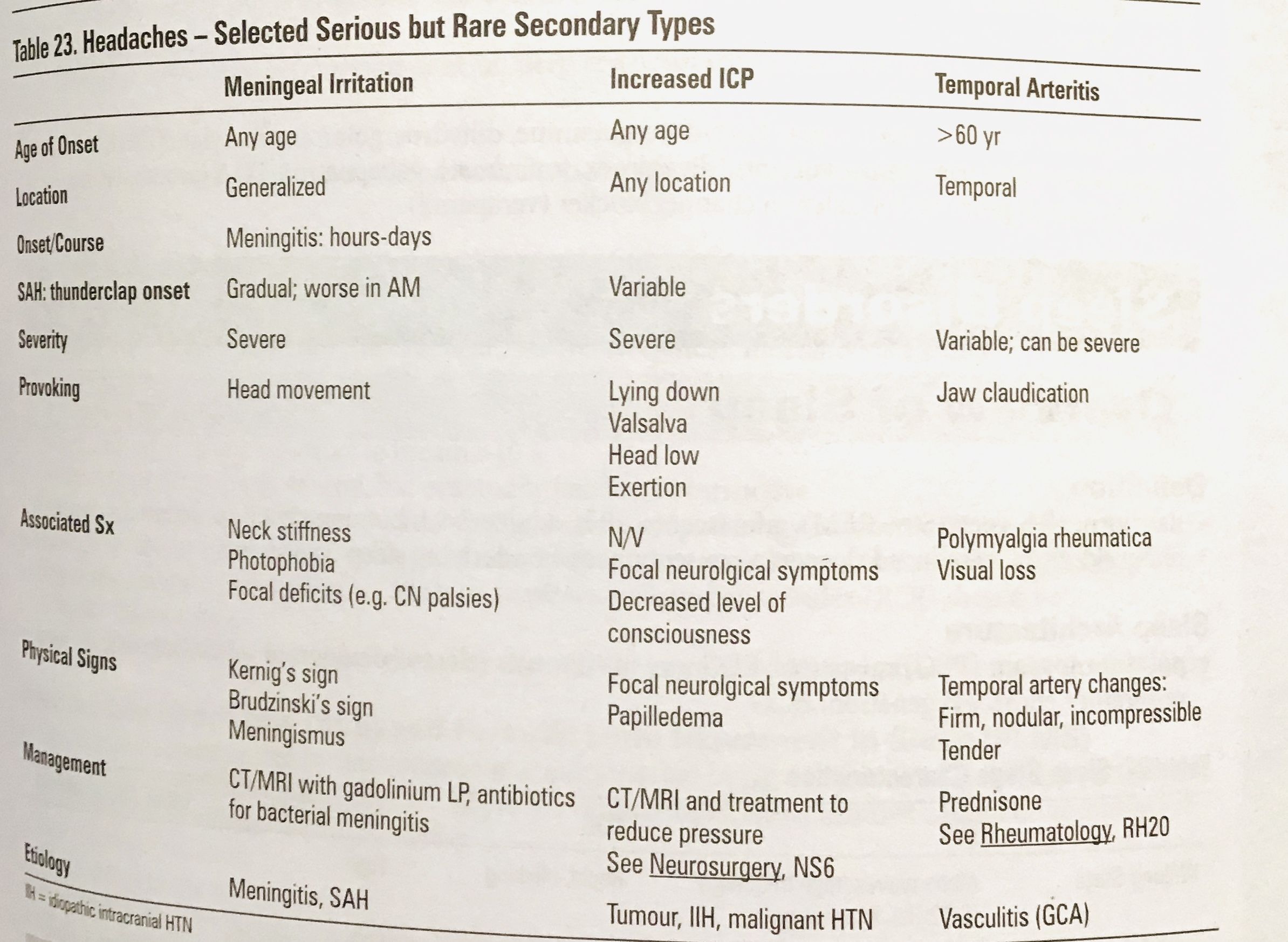
| Headache serious but rare secondary types | |
| History red flags in headache ( to consider CT / further investigation) | New onset (>50yr or < 5yr), quality - different /worse than the previous, sudden and severe (thunderclap), immunocompromised, fever, focal neurological deficits, head trauma |
| Physical exam red flags i. Headache | Papilledema, altered LOC, fever, meningismus, focal neurological deficit, signs of head trauma |
| Ottawa SAH rule | Have 100% sensitivity if <6hr onset, use for alert patients >15yr with new severe non traumatic headache reaching maximum intensity in less than 1hr. NOT for patients with new neurological deficits, previous aneurism, SAH, brain tumors or history of recurrent headache (>3in 6 mo) Investigate if >1: >40yr, neck pain or stiffness, witnessed loss of consciousness, onset during exertion, thunderclap headache, limited neck flex ion on examination |
| Management in patients with Headache suspicious of SAH or meningitis | If CT is negative ( >6hr onset) but clinically there is suspicion of SAH / meningitis perform LP and do not delay Abx and deliver first dose of dexamethasone with or before Abx |
| Red flags in back pain | “BACC PAIN” : B-bowel or bladder dysfunction, A-anesthesia (saddle), C-constitutional symptoms (cancer), C-chronic disease, P-paresthesia, A-age>50, I-infection or IV drugs abuse, N-neuromotorsdeficits |
| Clinical presentation of caudal equine syndrome (this is a surgical emergency) | Urinary retention followed by insensible urinary over flow, unrecognized fecal incontinence, distinct/loss of saddle Or perineal sensation |
| Indications for lumbar spine x-ray in back pain | ▪️No improvement after 6wks ▪️Fever >38 C ▪️Unexplained weight loss ▪️ Prolonged use of corticosteroid ▪️Significant trauma ▪️Progressive neurological deficit ▪️Suspicion of ankylosing spondylitis ▪️History of cancer (%metastasis) ▪️Alcohol/ drug abuse |
| Management of chronic, acute and subacute low back pain | ▪️Chronic >12 wks: analgesic (consider PPI if NSAID), low dose TCA, short term cyclobenzapine (for flare ups). Referral if red flags. Plus muscle relaxing massage, acupuncture, exercise and education. Moderate-severe pain: consider opioids and referral to multidisciplinary chronic pain program, epidural steroids, prolotherapy or surgery. ▪️ Acute and subacute: 70% resolves in 2wks 90%in 6wks, self care strategies, early return to work, physical activities and consider analgesics, reassess in 1-6 wks |
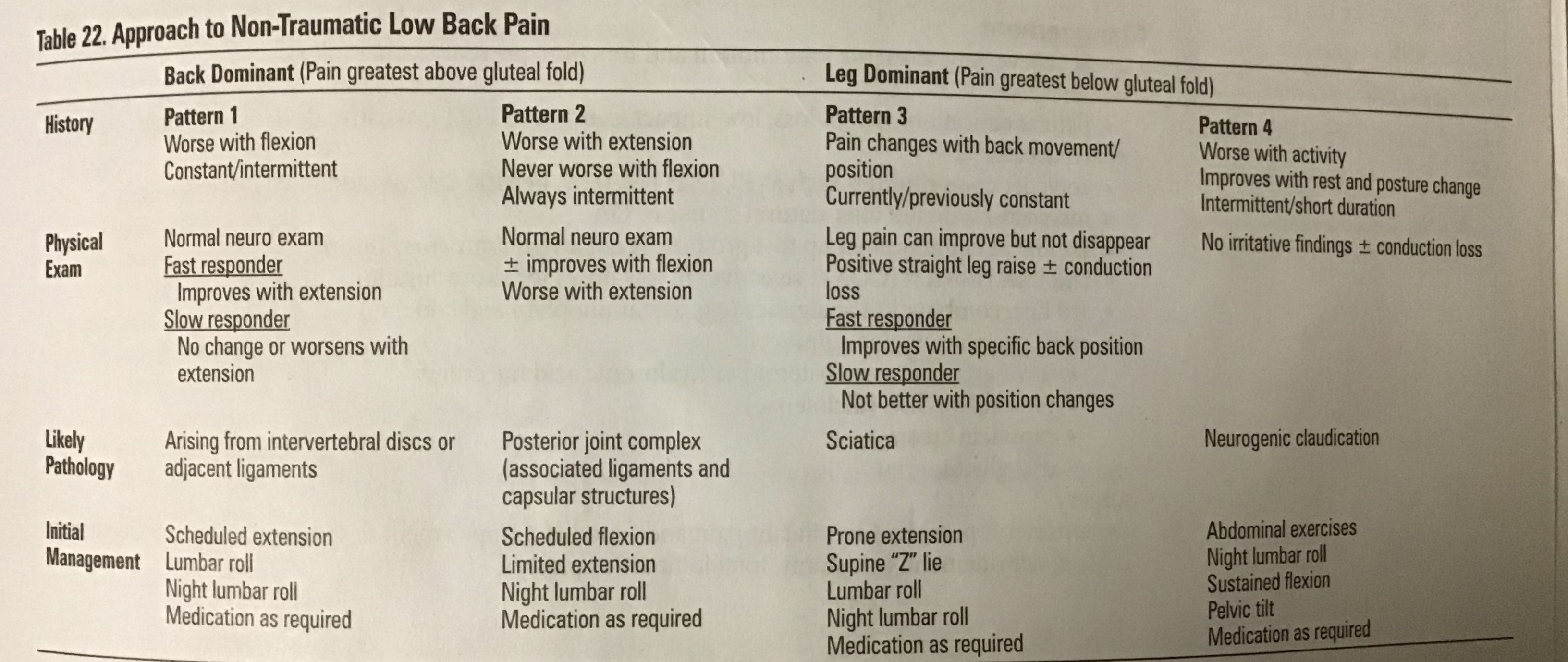
| Approach to non-traumatic low back pain | |
| Risk factors for osteoarthritis | Genetic predisposition, age, obesity (knees and hand), female, trauma |
| Investigations and findings in osteoarthritis | Normal Or negative : CBC, ESR, CRP, RF, ANA (OA it’s not an inflammatory disease) ▪️Hallmarks in radiology: 1.- joint space narrowing, 2.- subcondral sclerosis, 3.- subcondral cyst, 4.-osteophytes (Almost everyone >65yrs shows signs in x-ray but only 33% will be symptomatic) |
| General treatment in osteoarthritis | (No treatment alters the natural history of OA) 1#: acetaminophen 500mg tid(3gr/d max) 2# NSAIDs : ibuprofen 200-600mg tid, diclofenac 25-50 mg tid, diclofenac/misoprostol 50-75mg /200mgtid, naproxen 125-500 mg bid, meloxicam 7.5-15mg OD |
| Special treatment indications in osteoarthritis | ▪️Celecoxib 200mg/d in high risk of GI bleeding, 65yrs, Hx of GI bleed or PUD ▪️IA corticosteroids injections: short term (wks-mo), joint specific, decreased pain and improve function (rule out infection first) ▪️ IA hyaluronic acid: q6mo used for mild-moderate OA of the knees, crossed allergie with egg/chicken) |
| Contact dermatitis treatment | Wet compresses with burrows solution, barrier moisturizers and steroids. (Burrows solution its an aqueous solution of aluminum tricetate |
| Canadian prevalence of STI in clinical practice | ▪️Common: #1 chlamydia, #2 gonorrhea, HPV, Herpes ▪️non sexual: vulvovaginal candidiasis ( VVC), and bacterial vaginosis (BV) ▪️Most common infections associated with vaginal discharge: BV, VVC, trichomoniasis |
| Public health management in a STI | Offer hepatitis B vaccine, offer gardasil for women’s >9years (not covered for men in PH) , treat the partners |
| Mandatory reporting STI in canada | Chlamydia, gonorrhea, hepatitis a.b.c, HIV, Syphilis, (Others chancroid) CDC notifiable diseases. |
| Gonococcal urethritis/ cervicitis signs and symptoms, investigations, treatment and complications | ▪️S&S: M: urethral discharge, unexplained pyuria, dysuria, irritation, testicular swealling, sx of epididymitis, F: mucopurulent endocervical discharge, vaginal bleeding, dysuria, pelvic pain, dyspareunia. M&F: Often asymptomatic, can involve rectal symptoms in cases of unprotected anal sex ▪️Investigations: M: urethral swab for gram stain and culture (G- diplococcos) F: urine PCR, endocervical swab for gram stain and culture, vaginal swab for wet mount (to rule out trichomonas) ▪️Treatment: ceftriaxone 250 mg I.M. s.D. In risk factors for tax failure (pregnancy, pharyngeal, rectal infection) test of cure 4d after culture (#1) or urine PCR 2wks after (Alternative) ▪️ Complications: M: urethral strictures, epididymitis, infertility. F: PID, infertility, ectopic pregnancy, perinatal infection, M&F: arthritis (more common in men), risk of HIV. |
| Non gonococcal urethritis/ cervicitis (usually chlamydia) signs and symptoms, investigations, treatment and complications | Chlamydia its the most common bacterial STI in Canada, usually associated with N.gonorhoeae. ▪️S&S: 70-80% are asymptomatic, if symptoms appear are usually 2-6wks after infection and are similar to a gonococcal infection. ▪️Investigations: M: urethral swab for gram stain and culture (G- diplococcos) F: urine PCR, endocervical swab for gram stain and tissue culture (#1) or nuclei acid amplification test, vaginal swab for wet mount (to rule out trichomonas) ▪️Treatment: ceftriaxone 250 mg I.M. s.D.+ doxycycline 100 p.o. Bidx7d (not in pregnancy 2-3 trimester) or azithromycin 1gr. Test 3-4wks after in pregnancy P.o.s.d (#1)▪️ Complications: M: urethral strictures, epididymitis, infertility. F: PID, fits-Hugh-Curtis sx (liver capsule inflammation), infertility, ectopic pregnancy, perinatal infection, M&F: arthritis (more common in men), risk of HIV. |
| Human papilloma virus (genital warts,cervical dysplasia) Types | Most common viral STI in Canada ▪️Types: 6,11 are classically associated with anogenital warts/ condylomata acuminata, 16,18 are the most oncogenes (cervical HSIL) 16,18,31,33,35,36,45 are associated with increased incidence of cervical and Vulvar intraepithelial hyperplasia and carcinoma. |
| Human papilloma virus (genital warts,cervical dysplasia) signs and symptoms, investigations, treatment and prevention | ▪️S&s: Latent infection: most are asymptomatic, no visible lesions, only detected by dna hybridization test. Sub clinical: visible lesion found during colposcopy or Pap test. Clinical: visible wart-like lesion without magnification, hyperkeratonic, verrucous or flat macular lesion and valvular edema. ▪️Investigations: cytology, koilocytosis, biopsy of lesions at colposcopy, detection of HPV dna subtype using nucleic acid probes.▪️Treatment: patient administrated: Podofilox 0.5% solution/gel bidx3d in a row (4d off), then repeat x4wks, imiquimod (Aldara) 5% cream 3x/wk x 16wks. Provider administered: cryotherapy repeat q1-2wks, podophyllin resin in tincture of benzoin weekly, tri/bichloroacetic acid 80-90% weekly 4-6wks (safe in pregnancy), surgical remove /laser, intralesional interferon, in pregnancy: consider excision, c-section only if obstructing birth canal or risk of extensive bleeding, DoNOTUSE imiquimod,podophyllin, podofilox. ▪️Prevention: vaccination gardasil 9, gardasil (6,11,16,18), cervarix (16,18) |
| Herpes simplex virus (90% are type 2) signs and symptoms, investigations, treatment and complications | ▪️S&s: may be asymptomatic, initial symptoms present 2-21d after contact with prod oak symptoms like tingling, burning, pruritus, first episode with painful vesicoulcerative lesions and %fever,tender lymphadenopathy, dysuria and urinary retention only if urethral mucosa affected. Recurrent episodes are less extensive, shorter course and less frequent (usually only HSV-2). ▪️ Investigations: viral culture with swab of vesicular content, cytologic smear (tzanck smear), HSV Dna PCR ▪️Treatment: first episode acyclovir 200mg p.o. 5x/d x7-10d, famciclovir 250mg p.o. Tidx7-10d or valacyclovir 1gr p.o. Bid x7-10d, recurrent episode: acyclovir 200 mg p.o. 5x5d or 800mgp.o. Tid x2d, famciclovir 125 mg p.o. Bid x5d or valacyclovir 500mg p.o. Bid x3d or 1gr p.o./d x3d ▪️ Complications: genital pain, urethritis, cervicitis, aseptic meningitis, risk of HIV |
| Syphilis signs and symptoms, investigations and treatment | ▪️S&s: primary: 3-4 wk after exposure painless chancre and inguinal lymphadenopathy. Secondary: can resolve spontaneously, 2-6mo after initial infection, non specific symptoms, generalized maculopapular rash in palms, soles, trunk and limbs,condylomata anogenital, broad-based fleshy grey lesions. Tertiary may involve any organ system ▪️Investigations: aspiration of ulcers serum or node, dark field microscopy (#1) VDRL (non treponema test) is no reactive after treatment, the specific test is still reactivate for life. In primary serological test are usually negative, ▪️Benzathine penicillin G I.M. 2.4 mlls units S.D.for primary, secondary or latent (,<1 year) for >1 year latent use the same dose/wk x3 wks. Notify partners for he last 12mo. |
| Trichomoniasis (vulvovaginitis) signs and symptoms, investigation and treatment | ▪️S&S: 25% are asymptomatic, yellow-green,malodorous, diffuse, frothy discharge, petechiae on vagina and cervix, occasionally irritated ended vulva, dysuria and frequency, ph>4.5▪️Investigation: saline wet mount to see motile flagellated organism, WBC, PMN, can have positive amina test (whiff test) ▪️Even if asymptomatic use metronidazole 2gr P.O.S.D. ( Recommended in pregnancy) Or alternative 500mg P.O. Bid x7d. Treat partners |
| HIV diagnosis | Anti HIV antibodies detectable after a median of 3wks, virtually all by 3 mo, initial screening is with ELISA, (detects serum antibodies) A combination P24 antigen/HIV antibodies test used for screening in early acute infection and chronic infection (almost 100%Sn&Sp). The confirmatory test is the western blot (detects two different HIV protein bands) |
| HIV management | Always verify a positive test. Follow up every 3-6mo. Laboratory evaluation: order routine CD4 count if not stable/suppressed viral load (to see progress and stage of the disease), routine HIV-RNA levels (viral load) to see the rate of progression. ▪️Resistance test: HLA-B*5701 for abacavir hypersensitivity, CCR5 tropism. ▪️PPD>5cm (positive) serology ( hepatitisA,B,C CMV, VZV, syphilis, toxoplasma), biochemistry, hematology, CXR, urianalysis ▪️Initiate ART combination 2NRTI’s + 1INSTI/PI, until <40copies/ml (=undetectable %in 6mo) |
| Primary sleep disorders | Insomnia, narcolepsy, obstructive sleep apnea (OSA), restless leg syndrome or periodic limb movement |
| General management of sleep disorders | #1 CBT, #2 pharmacological treatment (short term) short acting benzodiazepines (lorazepam) non- benzodiazepines (zoplicone, zolpidem, melatonin), sedating antidepressants (amitriptyline, trazadone) |
| Restless leg syndrome and periodic limb movement etiology and management | Central ( spasticity), peripheral nervous system ( radiculopathy, neuropathy), pregnancy, iron deficit, alcohol intake ▪️First line dopaminergic agonist ( not Levo/carbidopa causes augmentation) |
| Sore throat red flags (pharyngitis) | >1 wk without improvement, respiratory difficulty, difficulty in handling secretions or swallowing ( peritonsillar abscess, ludwig’s angina), severe pain in the absence of erythema (Supra/epiglottitis), palpable mass (neoplasm), blood in the pharynx or ear (trauma) |
| Centor score for GABHS | ▪️+1: cough absent, Hx of fever, tonsillar exudate, swallen/ tender anterior nodes, age 3-14 years. ▪️0: age15-44 ▪️-1: Age>45 ▪️Score: 0-1 (1-2.5%-5-10%) no culture or Abx. Score 2-3 (11-17%-28-35%) culture all and treat with Abx only if positive. Score 4or more (51-53%) culture all, Abx on clinical grounds, discontinue if negative. |
| Infectious mononucleosis (EBV) management | Self limited course, symptomatic treatment, avoid heavy physical activities and contact sports for at least 1mo or until splenomegaly resolves due to de risk of splenic rupture. If acute airway obstruction give corticosteroids and referral to ENT. |
| Investigation in pharyngitis | In GABHS the gold standard is culture, rapid test forantigen have high specificity but low sensitivity. In mononucleosis peripheral blood smear, heterophile antibody test (latex agglutination or mono spot) |
| Community acquired pneumonia, outpatient without comorbidity patient treatment (S. Pneumoniae, M. Pneumoniae, C. Pneumoniae ) | ▪️1st amoxicillin 1000mg P.O. Tid x7-14d or clarithromycin 500mg PO. Bid x7-14d or azithromycin 500mg P.O. 1st day then 250mg P.O./d x4d or500mg x3d. ▪️2nd doxycycline 100mg P.O. X7-14d |
| Community acquired pneumonia, outpatient with comorbidity treatment (S. Pneumoniae, M. Pneumoniae, C. Pneumoniae + H. Influenzae ) | ▪️A B-lactam agent: Amoxicillin 1000mg/PO. Tid x14d or amo-clavulanate 500mg P.O. Tid or 875mg bid x7-14d or cefuroxime 500mg P.O. Bid x7-14d ▪️Plus one of: clarithromycin 500mg P.O.bid or 1000mg/d x7-14d or azithromycin 500mg P.O. The first day then 250mg/d x 4d or doxycycline 100mg p.o. Bid x 7-14d or any of the respiratory fluoroquinolones |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.